
POPULARITY

19 episodes with Acute coronary syndrome

15 episodes with Acute coronary syndrome

4 episodes with Acute coronary syndrome

2 episodes with Acute coronary syndrome

2 episodes with Acute coronary syndrome

5 episodes with Acute coronary syndrome

2 episodes with Acute coronary syndrome

3 episodes with Acute coronary syndrome

3 episodes with Acute coronary syndrome

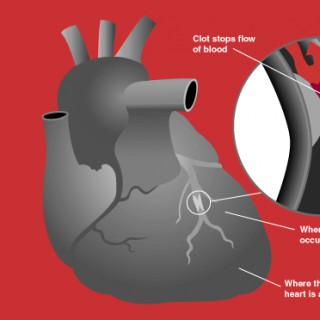
Acute Coronary Syndrome refers to a spectrum of conditions including Unstable Angina, Non ST Elevation Myocardial Infarction and ST Elevation Myocardial Infarction. In this video we look at the pathology behind acute coronary syndrome, the differences between Unstable angina, NSTEMI and STEMI, as well as the signs and symptoms, diagnosis (including ECG changes!) and treatment of each. PDFs available here: https://rhesusmedicine.com/pages/cardiologyConsider subscribing (if you found any of the info useful!): https://www.youtube.com/channel/UCRks8wB6vgz0E7buP0L_5RQ?sub_confirmation=1Buy Us A Coffee!: https://www.buymeacoffee.com/rhesusmedicineTimestamps:0:00 What is Acute Coronary Syndrome - Acute Coronary Syndrome Definition0:25 Coronary Artery Anatomy1:17 Acute Coronary Syndrome Pathology - Atherosclerosis 2:08 Acute Coronary Syndrome Pathology - Unstable Angina vs Non ST Elevation Myocardial Infarction vs ST Elevation Myocardial Infarction3:00 Acute Coronary Syndrome Risk Factors3:23 Signs and Symptoms of Acute Coronary Syndrome4:17 Acute Coronary Syndrome Diagnosis - ECG STEMI5:45 Acute Coronary Syndrome Diagnosis - ECG NSTEMI and Unstable Angina6:42 Acute Coronary Syndrome Diagnosis - Cardiac Troponin I 7:11 Acute Coronary Syndrome Diagnosis - Imaging7:42 Treatment of Acute Coronary SyndromeLINK TO SOCIAL MEDIA: https://www.instagram.com/rhesusmedicine/ReferencesBritish National Formulary (BNF), 2015. Acute coronary syndromes – treatment summary. [online] Available at: https://bnf.nice.org.uk/treatment-summary/acute-coronary-syndromes.html. BNFTeachMeAnatomy, 2025. Heart vasculature. [online] Available at: https://teachmeanatomy.info/thorax/organs/heart/heart-vasculature/. TeachMeAnatomy+1DeVon, H.A., 2020. Typical and atypical symptoms of acute coronary syndrome. Journal of the American Heart Association, 9:e015539. [online] Available at: https://www.ahajournals.org/doi/10.1161/JAHA.119.015539. AHA JournalsWarren, A., 2020. Acute coronary syndrome: risk factors, diagnosis and treatment. The Pharmaceutical Journal. [online] Available at: https://pharmaceutical-journal.com/article/ld/acute-coronary-syndrome-risk-factors-diagnosis-and-treatment. The Pharmaceutical JournalLife in the Fast Lane (LITFL), 2021. Acute coronary syndromes. [online] Available at: https://litfl.com/acute-coronary-syndromes/. Life in the Fast Lane • LITFLDisclaimer: Please remember this podcast and all content from Rhesus Medicine is for educational and entertainment purposes only and is not a guide to diagnose or to treat any form of condition. The content is not to be used to guide clinical practice and is not medical advice. Please consult a healthcare professional for medical advice.

New Study: Vitamin D Reduces Recurrent Heart Attacks by 50%? Ep. 1269 NOV 2025________________________________________Prevent Recurrent Heart Attacks, Targeted Vitamin D Dosing, Acute Coronary Syndrome Treatment, TARGET-D Trial Results 2025, Vitamin D Levels for Heart Health, Reducing MACE Risk, Intermountain Health Study.In this episode, we dive into the groundbreaking TARGET-D trial (presented at AHA 2025) that shows how "treating to target"—adjusting Vitamin D dosage to reach specific blood levels—may significantly reduce the risk of recurrent heart attacks. While the overall cardiovascular risk (MACE) didn't change statistically in the broad group, the study found a significant reduction in repeat heart attacks (Myocardial Infarction) for those in the treatment group. Learn the difference between "Intention to Treat" and "Per Protocol" analysis and what this means for secondary heart prevention.Source: May HT, Le VT, Anderson JL, et al. A Randomized Clinical Trial Evaluating Vitamin D Normalization on Major Adverse Cardiovascular-Related Events Among Acute Coronary Syndrome Patients: The TARGET-D Trial. Abstract presented at: American Heart Association Scientific Sessions 2025; November 9, 2025; New Orleans, LA.Disclaimers:• This information is for educational purposes only and should not be interpreted as medical advice.• The study discussed was conducted on Acute Coronary Syndrome patients (survivors of heart attack or unstable angina). These findings may not apply to the general healthy population.• Always consult with a qualified healthcare professional before making any changes to your diet, supplement regimen, or treatment plan.#VitaminD #HeartAttack #TARGETD #Cardiology #MedicalResearch________________________________________citation,TARGET-D trial,Vitamin D3 supplementation,Acute Coronary Syndrome,myocardial infarction reduction,heart attack prevention,treat to target vitamin D,cardiovascular health,25-hydroxyvitamin D,randomized clinical trial 2025,MACE outcomes,vitamin D deficiency,heart failure hospitalization,recurrent heart attack,vitamin D dosing algorithm,nutrition and heart disease,secondary prevention cardiology,vitamin D levels 40 ng/mL
Commentary by Dr. Jian'an Wang.
Commentary by Dr. Joon Ho Ahn.

This week on The Beat, CTSNet Editor-in-Chief Joel Dunning speaks with Dr. Anders Jeppsson, a cardiothoracic surgeon at Sahlgrenska University Hospital in Gothenburg, Sweden, about his paper on “Ticagrelor and Aspirin or Aspirin Alone After Coronary Surgery for Acute Coronary Syndrome,” published in The New England Journal of Medicine. Chapters 00:00 Intro 01:54 Ghana Mission Trip 06:23 JANS 1, Pig-to-Human Transplant 08:08 JANS 2, CABG Acute Type A AD 10:06 JANS 3, Chylothorax Lymph Node Management 11:22 JANS 4, ICU Resternotomy Adoption 13:38 JANS 5, Octogenarians Repair vs MV Surgery 15:10 Career Center 15:31 Video 1, MVR Patent Bilateral IMammary Grafts 16:36 Video 2, Repeat RA Thoracotomy 17:39 Video 3, Vascular Injuries in Robotics 19:12 Dr. Jeppsson Interview 33:30 EACTS 2025 & Upcoming Events They began by providing an overview of the study, including the reason for conducting it, the expansion of the study to other Nordic countries, and its results. They also discuss the funding for the research and the recruitment process. Additionally, they cover dual antiplatelet therapy and compare this study with similar research. Finally, they explore registry-based studies and future research on ticagrelor and aspirin, or aspirin alone, following coronary surgery for acute coronary syndrome. Joel also highlights recent JANS articles exploring whether protective coronary artery bypass grafting improves surgical outcomes in acute type A aortic dissection with coronary ostial involvement, the association of chylothorax with aggressiveness of lymph node management during pulmonary resection, if intensive care unit resternotomy should be practiced in all facilities that perform cardiac surgery, transcatheter edge-to-edge repair vs mitral valve surgery in octogenarians, and research using pig-to-human lung xenotransplantation into a brain-dead recipient. In addition, Joel explores robotic mitral valve replacement in a patient with patent bilateral internal mammary grafts, repeat right axillary thoracotomy as a safe and feasible approach for repair of recurrent LAVVR after previous AVSD repair, and handling vascular injuries in robotic thoracic surgery. Before closing, Joel highlights upcoming events in CT surgery. JANS Items Mentioned 1.) Protective Coronary Artery Bypass Grafting Improves Surgical Outcomes in Acute Type A Aortic Dissection With Coronary Ostial Involvement 2.) The Association of Chylothorax With Aggressiveness of Lymph Node Management During Pulmonary Resection 3.) Expert Opinion: Intensive Care Unit Resternotomy Should Be Practiced in All Facilities That Perform Cardiac Surgery 4.) Transcatheter Edge-to-Edge Repair Versus Mitral Valve Surgery in Octogenarians: Comparative Analysis of Safety, Durability, and Survival 5.) Pig-to-Human Lung Xenotransplantation Into a Brain-Dead Recipient CTSNet Content Mentioned 1.) Robotic Mitral Valve Replacement in a Patient With Patent Bilateral Internal Mammary Grafts: A Case Video 2.) Repeat Right Axillary Thoracotomy Is a Safe and Feasible Approach for Repair of Recurrent LAVVR After Previous AVSD Repair 3.) Handling Vascular Injuries in Robotic Thoracic Surgery: Real-Life Cases Using a Fibrin-Based Hemostatic Technique Other Items Mentioned 1.) Ticagrelor and Aspirin or Aspirin Alone After Coronary Surgery for Acute Coronary Syndrome 2.) Perfecting TAVR Removal | Skills Sharpening With Vince Gaudiani 3.) Career Center 4.) CTSNet Events Calendar Disclaimer The information and views presented on CTSNet.org represent the views of the authors and contributors of the material and not of CTSNet. Please review our full disclaimer page here.
The mechanism of action and safe administration of Morphine for patients with myocardial ischemia in ACLS's Acute Coronary Syndrome (ACS) algorithm.MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome.Morphine's use in the Acute Coronary Syndrome (ACS) algorithm.Why Morphine is helpful for patients with ACS.Contraindications and considerations for the safe administration of Morphine.Common dosing & administration of Morphine.Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration.Possible side effects of Morphine administration.Narcan as an antidote to Morphine if needed.**American Cancer Society (ACS) Fundraiser This is the seventh year that I'm participating in Men Wear Pink to increase breast cancer awareness and raise money for the American Cancer Society's life-saving mission.I hope you'll consider contributing.Every donation makes a difference in the fight against breast cancer! Paul Taylor's ACS Fundraiser Page: http://main.acsevents.org/goto/paultaylorTHANK YOU for your support! Good luck with your ACLS class!Links: Buy Me a Coffee at https://buymeacoffee.com/paultaylor Free Prescription Discount Card - Get your free drug discount card to save money on prescription medications for you and your pets: https://safemeds.vip/savePass ACLS Web Site - Other ACLS-related resources: https://passacls.com@Pass-ACLS-Podcast on LinkedIn
This week on The Beat, CTSNet Editor-in-Chief Joel Dunning speaks with Adanna Akujuo, a cardiothoracic surgeon and the surgical director of the Structural Heart Program at UVA Health University Medical Center, about the Voom Foundation and its trips to Africa. Chapters 00:00 Intro 01:39 Dr. Akujuo, Medical Missions 21:57 JANS 1, Ticagrelor and Aspirin Coronary 25:20 JANS 2, Long-Term MVR Durability Model 27:37 JANS 3, Duration of Donor Ventilation 29:18 JANS 4, Min Inv Concomitant Tri VR 31:40 JANS 5, Soft Robotic Artificial Hybrid Heart 33:32 Career Center 34:20 Video 1, RVOT Injury During Dissection 37:05 Video 2, Min Inv ASD Closure 38:31 Video 3, Redo AVR via Partial U Resternotomy 40:08 Upcoming Events 40:54 Closing They explore the foundation's goals, including training and educating local medical staff and providing essential care. Additionally, Dr. Akujo offers insights into the upcoming trip, discussing what a typical day entails, transportation logistics, accommodation, and the expenses that surgeons participating in the trip will need to cover, as well as what costs are taken care of by the foundation. The conversation also covers security measures in place, the average number of staff members on these trips, the daily surgical volume, and the most common cases. Joel also highlights recent JANS articles on which is best, ticagrelor and aspirin or aspirin alone after coronary surgery for acute coronary syndrome; an artificial intelligence and machine learning model for personalized prediction of long-term mitral valve repair durability; effect of duration of donor ventilation on lung transplant outcomes; surgical decision-making for concomitant tricuspid valve repair in minimally invasive mitral valve surgery; and a soft robotic total artificial hybrid heart. In addition, Joel explores right ventricular outflow tract injury during deep dissection in valve-sparing aortic root replacement, a minimally invasive approach for atrial septal defect closure, and redo aortic valve replacement via partial upper resternotomy. Before closing, Joel highlights upcoming events in CT surgery. JANS Items Mentioned 1.) Ticagrelor and Aspirin or Aspirin Alone After Coronary Surgery for Acute Coronary Syndrome 2.) An Artificial Intelligence and Machine Learning Model for Personalized Prediction of Long-Term Mitral Valve Repair Durability 3.) Effect of Duration of Donor Ventilation on Lung Transplant Outcomes 4.) Surgical Decision-Making for Concomitant Tricuspid Valve Repair in Minimally Invasive Mitral Valve Surgery 5.) A Soft Robotic Total Artificial Hybrid Heart CTSNET Content Mentioned 1.) Right Ventricular Outflow Tract Injury During Deep Dissection in Valve-Sparing Aortic Root Replacement 2.) Minimally Invasive Approach for Atrial Septal Defect Closure 3.) Redo Aortic Valve Replacement Via Partial Upper Resternotomy Other Items Mentioned 1.) Voom Foundation 2.) Career Center 3.) CTSNet Events Calendar Disclaimer The information and views presented on CTSNet.org represent the views of the authors and contributors of the material and not of CTSNet. Please review our full disclaimer page here.

Listen in as our expert panel discusses the latest recommendations for managing medications after heart attacks and other cardiac events. You'll hear our panelists review which antiplatelets to use, the optimal blood pressure meds, and the role of statin and non-statin cholesterol meds.Special guests:Danielle Blais, PharmD, FCCP, BCCP, BCPSCardiology Lead Specialty Practice PharmacistRichard M. Ross Heart HospitalThe Ohio State University Wexner Medical CenterJoel C. Marrs, PharmD, MPH., BCACP, BCCP, BCPS, FAHA, FASHP, FCCP, FNLAProfessor and Coordinator of Clinical OutreachThe University of Tennessee Health Science CenterDepartment of Clinical Pharmacy & Translational ScienceYou'll also hear practical advice from panelists on TRC's Editorial Advisory Board:Andrea Darby-Stewart, MDAssociate Director, Honor Health Family Medicine Residency ProgramClinical Professor of Family, Community & Occupational MedicineThe University of Arizona College of Medicine – PhoenixCraig D. Williams, PharmD, FNLA, BCPSClinical Professor of Pharmacy PracticeOregon Health and Science UniversityNone of the speakers have anything to disclose. This podcast is an excerpt from one of TRC's monthly live CE webinars, the full webinar originally aired in July 2025.TRC Healthcare offers CE credit for this podcast. Log in to your Pharmacist's Letter, Pharmacy Technician's Letter, or Prescriber Insights account and look for the title of this podcast in the list of available CE courses.Claim CreditThe clinical resources mentioned are part of a subscription to Pharmacist's Letter, Pharmacy Technician's Letter, and Prescriber Insights: Dual Antiplatelet Therapy for Coronary Artery DiseaseComparison of Oral Beta-BlockersAngiotensin Receptor Blockers and Angiotensin-Converting Enzyme InhibitorsCholesterol Guidelines (United States)Non-Statin Lipid-Lowering AgentsSend us a textIf you're not yet a subscriber, find out more about our product offerings at trchealthcare.com. Follow, rate, and review this show in your favorite podcast app. Find the show on YouTube by searching for ‘TRC Healthcare' or clicking here. You can also reach out to provide feedback or make suggestions by emailing us at ContactUs@trchealthcare.com.

Heart disease related costs in the United States amounted to nearly $239 billion between 2018 and 2019, and heart disease contributed to nearly 700,000 deaths. This activity will review the pathophysiology and clinical presentation of acute coronary syndromes and categorize the guideline-recommended pharmacologic management strategies for the treatment of unstable angina and acute myocardial infarction. These summaries will be supported by a review of the evidence that played a role in the development of these recommendations. CE for this episode expires two years after its original publication date. The information presented during the podcast reflects solely the opinions of the presenter. The information and materials are not, and are not intended as, a comprehensive source of drug information on this topic. The contents of the podcast have not been reviewed by ASHP, and should neither be interpreted as the official policies of ASHP, nor an endorsement of any product(s), nor should they be considered as a substitute for the professional judgment of the pharmacist or physician.
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome.Morphine's use in the Acute Coronary Syndrome (ACS) algorithm.Why Morphine is helpful for patients with ACS.Contraindications and considerations for the safe administration of Morphine.Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors.Common dosing & administration of Morphine.Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration.Possible side effects of Morphine administration.Narcan as an antidote to Morphine if needed.Good luck with your ACLS class!Links: Buy Me a Coffee at https://buymeacoffee.com/paultaylor Practice ECG rhythms at Dialed Medics - https://dialedmedics.com/Free Prescription Discount Card - Download your free drug discount card to save money on prescription medications for you and your pets: https://safemeds.vipPass ACLS Web Site - Episode archives & other ACLS-related podcasts: https://passacls.com@Pass-ACLS-Podcast on LinkedIn
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome.Morphine's use in the Acute Coronary Syndrome (ACS) algorithm.Why Morphine is helpful for patients with ACS.Contraindications and considerations for the safe administration of Morphine.Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors.Common dosing & administration of Morphine.Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration.Possible side effects of Morphine administration.Narcan as an antidote to Morphine if needed.Good luck with your ACLS class!Links: Buy Me a Coffee at https://buymeacoffee.com/paultaylor Practice ECG rhythms at Dialed Medics - https://dialedmedics.com/Free Prescription Discount Card - Download your free drug discount card to save money on prescription medications for you and your pets: https://safemeds.vipPass ACLS Web Site - Episode archives & other ACLS-related podcasts: https://passacls.com@Pass-ACLS-Podcast on LinkedIn

Send us a textToday we're introducing a new format—the first episode in our Clinical Practice Guidelines series. This week, Drs. Mike and John Fralick discuss the 2025 ACC/AHA Clinical Practice Guidelines for Acute Coronary Syndrome. Here we go! Support the show

Send us a textWelcome back Rounds Table Listeners! Today we're introducing a new format—the first episode in our Clinical Practice Guidelines series. This week, Drs. Mike and John Fralick discuss the 2025 ACC/AHA Clinical Practice Guidelines for Acute Coronary Syndrome. Here we go!2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes (0:00 - 18:56)Mike's interview with Dr. Jeff Carson:Episode 110 - Restrictive versus Liberal Transfusion in Myocardial Infarction with Dr. Jeff CarsonThe Good Stuff:Egg cracking tips! (18:57 - 19:47)Jerro (19:48 - 20:47)Questions? Comments? Feedback? We'd love to hear from you! @roundstable @InternAtWork @MedicinePods
Darshan H. Brahmbhatt, Podcast Editor of JACC: Advances, discusses a recently published original research paper on Apixaban Dose in Patients With Atrial Fibrillation and Acute Coronary Syndrome and/or Undergoing Percutaneous Coronary Intervention: Insights From AUGUSTUS.
Mirza Umair Khalid, MD, social media editor of JACC: Cardiovascular Interventions, and William F. Fearon, MD, FACC, discuss analysis from FAME III trial comparing outcomes of CABG vs FFR-guided multivessel PCI for patients in ACS versus CCS.

Justin Coleman speaks with Kate Ziser, a pharmacist at the Princess Alexandra Hospital in Brisbane, about her paper on the role of triple antithrombotic therapy in patients with atrial fibrillation following coronary stent insertion. Kate explains when triple therapy is indicated, the duration of therapy, and the step-down approach to antithrombotic therapy. Read the full article by Kate and her co-authors in Australian Prescriber.

Antithrombotic Therapy in ACS
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome or ACS. Morphine's use in the Acute Coronary Syndrome (ACS) algorithm. Why Morphine is helpful for patients with ACS. Contraindications and considerations for the safe administration of Morphine. Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors. Common dosing & administration of Morphine. Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration. Possible side effects of Morphine administration. Narcan as an antidote to Morphine if needed.Connect with me:Website: https://passacls.com@Pass-ACLS-Podcast on LinkedInGive Back & Help Others: Your support helps cover the monthly cost of software and podcast & website hosting. Donations at Buy Me a Coffee at https://buymeacoffee.com/paultaylor are appreciated and will help ensure others can benefit from these tips as well.Good luck with your ACLS class!Helpful Listener Links:Practice ECG rhythms at Dialed Medics - https://dialedmedics.com/
This episode of JACC-Baran features a brief discussion on Kendrick Lamar and the history of racial discrimination in the United States. Then Hiroki Ueyama, MD, from Emory University discusses his study on P2Y12 inhibitor pre-treatment in NST-ACS using data from the Chest Pain-MI Registry. The study examines how guideline changes have influenced clinical practice, revealing a decline in pre-treatment rates, significant practice variations, and no major differences in outcomes except for longer hospital stays in CABG patients. Watch the video or listen as a podcast here, then check out the JACC article: https://www.jacc.org/doi/10.1016/j.jacc.2024.09.1227
In this podcast, Dr. Valentin Fuster discusses a study on the use of P2Y12 inhibitor pretreatment in patients with non-ST elevation acute coronary syndrome, revealing significant variability in its application across institutions and operators. Despite initial hypotheses of benefit, the findings indicate no significant difference in patient outcomes, suggesting that routine pretreatment may not be necessary, especially when treatment is initiated within 24 hours of symptom onset.
Join us as Monee and Meredith with the rest of the hospital medicine team reflect on the past year, discussing some favorite insights gained covering a range of topics, including diabetic foot infections, sepsis, sickle cell inpatient management, syncope, psychiatry for the hospitalist, and acute coronary syndrome. No CME for this episode, but claim CME for past shows at curbsiders.vcuhealth.org! Patreon | Episodes | Subscribe | Spotify | YouTube | Newsletter | Contact | Swag! | CME Show Segments Introduction Picks of the Year Diabetic Foot Infections Sepsis Sickle Cell Inpatient Management Psychiatry Primer Syncope Acute Coronary Syndrome Reflections from the Year Credits Written, Produced, and hosted by: Meredith Trubitt MD; Monee Amin MD Script Written: Caroline Coleman, MD, RJ Blackburn, MD Cover Art: Caroline Coleman, MD Reviewer: Rahul Ganatra MD Showrunners: Matthew Watto MD, FACP; Paul Williams MD, FACP Technical Production: PodPaste Sponsor: Rosetta Stone Redeem your 50% off at rosettastone.com/curbsiders
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome or ACS. Morphine's use in the Acute Coronary Syndrome (ACS) algorithm. Why Morphine is helpful for patients with ACS. Contraindications and considerations for the safe administration of Morphine. Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors. Common dosing & administration of Morphine. Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration. Possible side effects of Morphine administration. Narcan as an antidote to Morphine if needed.Connect with me:Website: https://passacls.com@Pass-ACLS-Podcast on LinkedInGive Back & Help Others: Your support helps cover the monthly cost of software and podcast & website hosting so that others can benefit from these ACLS tips as well. Donations via Buy Me a Coffee at https://buymeacoffee.com/paultaylor are appreciated.Good luck with your ACLS class!

Maddy, Youssef and Andrew share their approach to acute coronary syndrome as they discuss a case presented by Sharmin. Acute Coronary Syndrome Framework To join us live on Virtual Morning Report (VMR), sign up HERE. Download CPSolvers App here RLRCPSOLVERS
JACC Associate Editor Seng Chan You, MD, and author Hiroki Ueyama, MD discuss this study presented at AHA and published in JACC. NCDR study finds a steady decline in P2Y12 inhibitor pretreatment for NSTE-ACS in the US, but significant variability persists among operators, institutions, and regions. This practice was not associated with any benefits but was linked to a longer length of stay among those undergoing CABG, underscoring the importance of maintaining efforts to integrate evidence into clinical practice.
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome or ACS. Morphine's use in the Acute Coronary Syndrome (ACS) algorithm. Why Morphine is helpful for patients with ACS. Contraindications and considerations for the safe administration of Morphine. Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors. Common dosing & administration of Morphine. Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration. Possible side effects of Morphine administration. Narcan as an antidote to Morphine if needed.Connect with me:Website: https://passacls.com@Pass-ACLS-Podcast on LinkedInGive Back & Help Others: Your support helps cover the monthly cost of software and podcast & website hosting so that others can benefit from these ACLS tips as well. Donations made via Buy Me a Coffee at https://buymeacoffee.com/paultaylor are appreciated.Make a difference in the fight against breast cancer by donating to my Men Wear Pink fundraiser for the American Cancer Society (ACS) at http://main.acsevents.org/goto/paultaylor Every dollar helps in the battle with breast cancer.Good luck with your ACLS class!
Darshan H. Brahmbhatt, Podcast Editor of JACC: Advances discusses a recently published original research paper on machine-learning for phenotyping and prognostication of myocardial infarction and injury in suspected acute coronary syndrome.
Quit playing games with my heart Yet another beat no to skip here with part 2 of our conversation with cardiologist Dr. Sanjeev Francis (@, Maine Medical Center)for acute coronary syndrome. Learn about the warranty on stress tests, initial management of ACS and how to deal with those pesky elevated troponins from patients with sepsis. Claim CME for this episode at curbsiders.vcuhealth.org! Patreon | Episodes | Subscribe | Spotify | YouTube | Newsletter | Contact | Swag! | CME Show Segments Start Part 1 Intro Rapid fire questions/Picks of the Week Case 1 History and Physical ECGs Definitions Risk Stratification Tools Non-invasive Testing Options End Part 1 Start Part 2 Case 2 Warranty on Non-invasive Testing Invasive Management of non ST elevation ACS Medical Management of non ST elevation ACS Case 3 Myocardial Injury Definitions Diagnostics to Consider for Myocardial Injury Transitions of Care Outro End Part 2 Credits Producer, Writer, Show Notes, Hosts: Meredith Trubitt, MD, MPH, Monee Amin MD Infographic, Cover Art: Caroline Coleman, MD Reviewer: Rahul Ganatra, MD, MPH Showrunners: Matthew Watto MD, FACP; Paul Williams MD, FACP Technical Production: PodPaste Guest: Sanjeev Francis, MD Sponsor: Babbel Get up to 60% off your Babbel subscription - but only for our listeners at Babbel.com/CURB. Sponsor: Freed You can try Freed for free right now by going to freed.ai. And listeners of Curbsiders can use code CURB50 for $50 off their first month. Sponsor: Panacea Financial If you're ready to join the thousands of doctors who have declared independence from traditional banks, visit panaceafinancial.com today.
In the September 10, 2024, issue of JACC, the study by Dr. Doron Seeker and colleagues investigates alirocumab's impact on cardiovascular outcomes related to triglyceride levels. Despite effectively lowering LDL cholesterol, alirocumab did not show significant clinical benefit through triglyceride reduction, suggesting that its efficacy may be limited in addressing cardiovascular risk associated with elevated triglycerides.
Don't skip a beat and join us in part 1 of our conversation with cardiologist Dr. Sanjeev Francis (@, Maine Medical Center)for acute coronary syndrome. First up, the basics on physical exam, how to interpret high-sensitivity troponin and how to think through the spectrum of acute coronary syndrome. Claim CME for this episode at curbsiders.vcuhealth.org! Patreon | Episodes | Subscribe | Spotify | YouTube | Newsletter | Contact | Swag! | CME Show Segments Start Part 1 Intro Rapid fire questions/Picks of the Week Case 1 History and Physical ECGs Definitions Risk Stratification Tools Non-invasive Testing Options End Part 1 Start Part 2 Case 2 Warranty on Non-invasive Testing Invasive Management of non ST elevation ACS Medical Management of non ST elevation ACS Case 3 Myocardial Injury Definitions Diagnostics to Consider for Myocardial Injury Transitions of Care Outro End Part 2 Credits Producer, Writer, Show Notes, Hosts: Meredith Trubitt, MD, MPH, Monee Amin MD Infographic, Cover Art: Caroline Coleman, MD Reviewer: Rahul Ganatra, MD, MPH Showrunners: Matthew Watto MD, FACP; Paul Williams MD, FACP Technical Production: PodPaste Guest: Sanjeev Francis, MD Sponsor: Mint Mobile To get your new 3-month premium wireless plan for just 15 bucks a month, go to mintmobile.com/CURB. Sponsor: Freed You can try Freed for free right now by going to freed.ai. And listeners of Curbsiders can use code CURB50 for $50 off your first month. Sponsor: American College of Physicians Preorder ACP MKSAP to receive discounted pricing plus free MKSAP 19 premium content you can use now at acponline.org/acpmksap
In this CCO Nephrology podcast episode, hear from cardiologist Erin D. Michos, MD, MHS, FACC, FAHA, FASE, FASPC, and nephrologist Mark J. Sarnak, MD, MS, as they explore the pathophysiology and novel therapeutic strategies to target residual inflammatory risk associated with ASCVD and CKD. Episode outline: Moving beyond lipid lowering to address residual inflammatory riskNovel anti-inflammatory targets for ASCVD To learn more about targeting residual risk associated with systemic inflammation, find more educational activities and resources with the links below: CME-certified text module with animated pathophysiology video and faculty voice audio clipsClinicalThought commentariesPodcast episode 1, discussing residual risk associated with systemic inflammation and the role of cardiologists and nephrologists in mitigating risk in ASCVD and CKD Podcast episode 3, featuring faculty discussion of new and emerging therapies to target inflammatory risk in patients with ASCVD and CKD
In this CCO Nephrology podcast episode, hear from cardiologist Erin D. Michos, MD, MHS, FACC, FAHA, FASE, FASPC, and nephrologist Mark J. Sarnak, MD, MS, as they explore new and emerging strategies to target residual risk associated with systemic inflammation in patients with ASCVD and CKD. Episode outline: The relationship among systemic inflammation, ASCVD, and CKD The role of cardiologists and nephrologists in screening and mitigating systemic inflammation To learn more about targeting residual risk associated with systemic inflammation, find more educational activities and resources with the links below: CME-certified text module with animated pathophysiology video and faculty voice audio clips ClinicalThought commentaries Podcast episode 2, discussing novel therapeutic approaches to address residual inflammatory risks in patients with ASCVD and CKD Podcast episode 3, featuring faculty discussion of new and emerging therapies to target inflammatory risk in patients with ASCVD and CKD
In this CCO Nephrology podcast episode, hear from cardiologist Erin D. Michos, MD, MHS, FACC, FAHA, FASE, FASPC, and nephrologist Mark J. Sarnak, MD, MS, as they discuss new and emerging therapies designed to target residual inflammatory risk associated with ASCVD and CKD. Episode outline: Colchicine: inhibition of NLRP3 inflammasome assembly/activationCanakinumab (anti–IL-1β monoclonal antibody)Ziltivekimab (anti–IL-6 monoclonal antibody)Other emerging targets/therapies To learn more about targeting residual risk associated with systemic inflammation, find more educational activities and resources with the links below: CME-certified text module with animated pathophysiology video and faculty voice audio clips ClinicalThought commentaries Podcast episode 1, discussing residual risk associated with systemic inflammation and the role of cardiologists and nephrologists in mitigating risk in ASCVD and CKD Podcast episode 2, discussing novel therapeutic approaches to address residual inflammatory risks in patients with ASCVD and CKD
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome or ACS. Morphine's use in the Acute Coronary Syndrome (ACS) algorithm. Why Morphine is helpful for patients with ACS. Contraindications and considerations for the safe administration of Morphine. Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors. Common dosing & administration of Morphine. Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration. Possible side effects of Morphine administration. Narcan as an antidote to Morphine if needed.Connect with me:Website: https://passacls.com@PassACLS on X (formally known as Twitter)@Pass-ACLS-Podcast on LinkedInGive back & help others. Your support will help cover the monthly cost of software and podcast & website hosting. Donations made via Buy Me a Coffee at https://buymeacoffee.com/paultaylor are appreciated.Good luck with your ACLS class!

Get full access to Cardiology Trial's Substack at cardiologytrials.substack.com/subscribe
Commentary by Dr. Valentin Fuster

Acute Assessment Of Patients With High Cardiovascular Risk Post-acute Coronary Syndrome (TELE-ACS)
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome or ACS. Morphine's use in the Acute Coronary Syndrome (ACS) algorithm. Why Morphine is helpful for patients with ACS. Contraindications and considerations for the safe administration of Morphine. Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors. Common dosing & administration of Morphine. Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration. Possible side effects of Morphine administration. Narcan as an antidote to Morphine if needed.Connect with me:Website: https://passacls.com@PassACLS on X (formally known as Twitter)@Pass-ACLS-Podcast on LinkedInGive back - buy Paul a bubble tea hereGood luck with your ACLS class!
Ticagrelor Monotherapy in Patients with Acute Coronary Syndrome: An Individual Patient Data Meta-Analysis of Randomized TICO and T-PASS Trials
Note to readers: Since going live with Cardiology Trials Substack in January of 2024 we have been exclusively covering trials that we have categorized as belonging to the major subject heading “Acute Coronary Syndrome” belonging to the subsection “Medicines”. Our indexing scheme was described in one of our original posts and we encourage our audience to read it if you have not already. This is pertinent because the next several trials being presented may seem to come out of the blue but we assure you there is a method.N Engl J Med 2007;357:2011-15.Background Up to now we have presented trials involving major foundational medical therapies for acute coronary syndrome which include aspirin, thrombolytic agents and anticoagulation, but not those involving percutaneous coronary intervention (PCI) as they are reserved for another section. But, by the turn of the 21st century, PCI had become the dominant up-front strategy for revascularization in many countries around the world. Clinical trials demonstrated it improved outcomes, the main one being re-infarction, compared to thrombolysis in patients with STEMIs, and there was an evolving evidence for it in non-ST-segment elevation acute coronary syndrome (STEACS) as well, where thrombolysis had not demonstrated any significant benefits.As PCI became dominant, antithrombotic strategies for optimizing outcomes following PCI evolved along with it. These early trials generally involved a mixture of patient phenotypes (acute vs elective PCI) and were relatively small and of limited quality by comparison to many of the seminal trials presented thus far. Instead of presenting each of these smaller studies, we direct readers to a narrative review that nicely describes the evolution of dual-antiplatelet therapy for PCI and other indications.Briefly: dual-antiplatelet therapy with aspirin and ticlopidine, an antiplatelet agent belonging to the drug class of thienopyridines, which inhibits platelet aggregation induced by ADP, was found superior to aspirin alone or aspirin plus anticoagulation when PCI was performed; however, there were concerns about its safety. Clopidogrel was developed after ticlopidine; it had a similar mechanism of action but less safety concerns and could be given as a loading dose to produce more rapid effects. Despite limited evidence from clinical trials comparing it head-to-head with ticlopidine it became the dominant thienopyridine agent on the market and still has a prominent role in the management of cardiovascular diseases today.Following PCI and dual-antiplatelet therapy with aspirin and clopidogrel, patients continue to have an elevated risk of coronary events, in general, and in-stent related coronary events, in particular. Some of this risk has been attributed to limitations of clopidogrel itself. Clopidogrel has modest antiplatelet effects (compared to other thienopyridines) with substantial interpatient variability due to genetic polymorphisms that impact clopidogrel metabolism and antiplatelet efficacy. Clopidogrel also has a delayed onset of action, which is especially relevant regarding its ability to protect against the dreaded adverse event of early in-stent thrombosis.Prasugrel is a thienopyridine—developed after clopidogrel—that inhibits platelet aggregation more rapidly, consistently and to a greater extent. The Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial Infarction (TRITON–TIMI) 38 trial sought to test the hypothesis that prasugrel would reduce major cardiovascular events compared to clopidogrel in patients with acute coronary syndrome undergoing PCI.Cardiology Trial's Substack is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.Patients Eligible patients had either moderate-to-high risk unstable angina (UA) or NSTEMI or STEMI. UA and NSTEMI were defined by ischemic symptoms lasting 10 minutes or more and occurring within 72 hours before randomization, a TIMI risk score of 3 or more, and either ST-segment deviation of 1 mm or more or elevated levels of a cardiac biomarker of necrosis. STEMI was traditionally defined. Key exclusion criteria included an increased risk of bleeding, anemia, thrombocytopenia, a history of pathologic intracranial findings, or the use of any thienopyridine within 5 days before enrollment.Baseline characteristics The median age of patients was 61 years with 13% being ≥75 years and 74% were men; over 90% were white. The index event was UA or NSTEMI in 74% and STEMI in 26%. PCI was performed in 99% of patients and split evenly between those receiving bare metal or drug eluting stent(s). 18% of patients had a prior MI, 23% had diabetes, 64% had hypertension and 38% were tobacco users. Only 11% of patients had CKD defined as a creatinine clearance ≤60 ml/min.Procedures A loading dose of prasugrel 60 mg or clopidogrel 300 mg was given in a double blind manner anytime between randomization up to 1 hour after leaving the catheterization laboratory. In order to be randomized, the plan for PCI had to be known. This could occur before going to the cath lab for planned PCI, if the anatomy was already known or occur in the cath lab during the case where anatomy was determined and PCI was performed. If PCI was planned, patients were eligible to undergo pretreatment with the study drug for up to 24 hours prior to PCI.Treating physicians determined the vessels treated, devices used, and adjunctive medication administered to support PCI. After PCI, patients received maintenance doses of either prasugrel 10 mg daily or clopidogrel 75 mg daily. Use of aspirin at a dose of 75 to 162 mg daily was recommended. Study visits were conducted at hospital discharge, 30 days, 90 days, and 3-month intervals thereafter, for a total of 6 to 15 months.Endpoints The primary efficacy endpoint was a composite of cardiovascular death, nonfatal MI or stroke during the follow up period. A prespecified “landmark” analysis was undertaken to compare the primary endpoint event rate up to 3 days following randomization and from day 3 to the end of the study. The sample size calculation was event-driven and it was determined that 875 primary endpoint events would provide 90% power to detect a relative risk reduction of 20%. A prespecified analysis performed after 650 events revealed a lower than anticipated event rate and the investigators increased the sample size accordingly.Results A total of 13,608 patients (10,074 with UA or NSTEMI and 3534 with STEMI), from 707 sites in 30 countries were enrolled. There were 6,813 patients assigned to the prasugrel group and 6,795 assigned to clopidogrel. The median duration of therapy was 14.5 months. Prasugrel significantly reduced the primary composite endpoint compared to clopidogrel (9.9% vs 12.1%; HR 0.81; 95% CI 0.73-0.90; P
Pre-Hospital Rule-Out of Non-ST-Segment Elevation Acute Coronary Syndrome by a Single Troponin Measurement: Final One-Year Outcomes of the ARTICA Randomised Trial (AHA 2023)
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome or ACS. Morphine's use in the Acute Coronary Syndrome (ACS) algorithm. Why Morphine is helpful for patients with ACS. Contraindications and considerations for the safe administration of Morphine. Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors. Common dosing & administration of Morphine. Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration. Possible side effects of Morphine administration. Narcan as an antidote to Morphine if needed. Connect with me:Website: https://passacls.com@PassACLS on X (formally known as Twitter)@Pass-ACLS-Podcast on LinkedInGive back via PayPal Good luck with your ACLS class!

Looking for more information on this topic? Check out the Drugs to Treat Acute Coronary Syndrome brick. If you enjoyed this episode, we'd love for you to leave a review on Apple Podcasts. It helps with our visibility, and the more med students (or future med students) listen to the podcast, the more we can provide to the future physicians of the world. Follow USMLE-Rx at: Facebook: www.facebook.com/usmlerx Blog: www.firstaidteam.com Twitter: https://twitter.com/firstaidteam Twitter: https://twitter.com/mesage_hub Instagram: https://www.instagram.com/firstaidteam/ YouTube: www.youtube.com/USMLERX Learn more about Rx Bricks by signing up for a free USMLE-Rx account: www.usmle-rx.com You will get 5 days of full access to our Rx360+ program, including over 800 Rx Bricks. After the 5-day period, you will still be able to access over 150 free bricks, including the entire collections for General Microbiology and Cellular and Molecular Biology.

With the expertise of top cardiologists and medical researchers Dr. Michael Koren and Dr. Miciah Jones we follow up on the October 18, 2023 podcast Exploring Cardiac Health: Acute Coronary Syndrome, Gender Differences, and Cholesterol Management Ep 148. We uncover the truth about Plavix and its role in treating, not preventing, heart disease. We also shed light on the overlooked signs of heart disease in women and how the medical community is stepping up its game in diagnosis. Dive into hospital procedures for heart attack assessment and the potential lifelong use of cholesterol drugs.Ever wondered about the complexities of stress testing in heart disease diagnosis? We unravel these intricacies, discuss the pros and cons of various tests, and emphasize the importance of collaborating with the right healthcare professionals. Highlighting how a deep understanding of your body's anatomy and physiology can help detect potential health issues, we walk you through the labyrinth of diagnostic options. Don't miss out on this enlightening and potentially life-saving discussion as we delve into heart disease and its management.Be a part of advancing science by participating in clinical researchShare with a friend. Rate, Review, and Subscribe to the MedEvidence! podcast to be notified when new episodes are released.Follow us on Social Media:FacebookInstagramTwitterLinkedIn Powered by ENCORE Research GroupMusic: Storyblocks - Corporate InspiredThank you for listening!
Are you prepared for a journey into the fascinating world of cardiac health? We promise you insights that could be life-altering. Dr. Michael Koren and Dr. Miciah Jones illuminate us on acute coronary syndrome and the immediate benefits of high-dose statin medication. Their expertise in diet, exercise, prevention, and procedural therapy provides a holistic perspective on coronary artery disease. We then channel our focus to the often-overlooked topic of gender differences in heart disease. With women presenting more vague symptoms and experiencing higher complications when treated for a STEMI, it's a conversation that is crucial now more than ever. Join us as we traverse this critical landscape, exploring the alarming trend of plateauing progress in reducing cardiovascular deaths in the United States. It's an engaging discourse that serves as a call to action for us all to work towards reducing deaths from heart disease.As we wrap up this episode, we demystify the complexities of cholesterol. Shedding light on the contrasting roles of LDL and HDL cholesterol. The significance of managing cholesterol levels, and we talk about how physical activity and statins are allies in this fight. Our segment on the potential side effects of statins and ways to minimize the residual risk of cardiovascular disease is not to be missed. So, tune in! We guarantee you'll walk away with a wealth of knowledge and practical tips for a heart-healthy lifestyle.Rebroadcast from September 6, 2023, WJCT Sip & Science eventBe a part of advancing science by participating in clinical researchShare with a friend. Rate, Review, and Subscribe to the MedEvidence! podcast to be notified when new episodes are released.Follow us on Social Media:FacebookInstagramTwitterLinkedIn Powered by ENCORE Research GroupMusic: Storyblocks - Corporate InspiredThank you for listening!

Dear folks, as you know ESC 2023 acute coronary syndrome guideline has many new concepts, we decided to summarize its content and we hope you will enjoy listening to this episode. You can also download the slide set prepared by ESC by clicking the following link:http://ecardiocast.com/wp-content/uploads/2023/10/ACS-Guideline.pdf
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome or ACS. Morphine's use in the Acute Coronary Syndrome (ACS) algorithm. Why Morphine is helpful for patients with ACS. Contraindications and considerations for the safe administration of Morphine. Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors. Common dosing & administration of Morphine. Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration. Possible side effects of Morphine administration. Narcan as an antidote to Morphine if needed.**American Cancer Society (ACS) Fundraiser This is the fifth year that I'm participating in Men Wear Pink to increase breast cancer awareness and raise money for the American Cancer Society's life-saving mission.I hope you'll consider contributing.Every donation makes a difference in the fight against breast cancer! Paul Taylor's ACS FundraiserTHANK YOU! Connect with me:Website: https://passacls.com@PassACLS on Twitter@Pass-ACLS-Podcast on LinkedInGive back & support the show:via PayPal Good luck with your ACLS class!
MONA is the acronym sometimes used to help us remember the interventions to consider for patients with Acute Coronary Syndrome or ACS. Morphine's use in the Acute Coronary Syndrome (ACS) algorithm. Why Morphine is helpful for patients with ACS. Contraindications and considerations for the safe administration of Morphine. Morphine as an alternative to nitro for patients with chest pain that take PDE inhibitors. Common dosing & administration of Morphine. Monitoring of the patient's level of consciousness, pain, blood pressure, and respirations after administration. Possible side effects of Morphine administration. Narcan as an antidote to Morphine if needed.Connect with me:Website: https://passacls.com@PassACLS on Twitter@Pass-ACLS-Podcast on LinkedInGive back & support the show:via PayPal Good luck with your ACLS class!

In this episode of Curbside Consults, we examine the 2022 scientific statement from the American Heart Association on the management of acute coronary syndrome in the older adult population. We are joined by Dr. Abdulla Damluji, the lead author on the scientific statement. Dr. Damluji is an interventional cardiologist at Inova Heart and Vascular Institute and Associate Professor of Medicine at Johns Hopkins University School of Medicine.

This episode covers acute coronary syndrome.Written notes can be found at https://zerotofinals.com/medicine/cardiology/acs/ or in the cardiology section of the 2nd edition of the Zero to Finals medicine book.The audio in the episode was expertly edited by Harry Watchman.

The Pharm So Hard Podcast: An Emergency Medicine and Hospital Pharmacy Podcast
While still new, emergency medicine pharmacists and pharmacotherapy has not had its own platform to present the latest evidence and issues facing emergency medicine pharmacy, until now. The EmpoweRx Conference, to be held in concurrently with the SAEM Annual Meeting, is designed by practicing emergency medicine pharmacists. The program will include a multidisciplinary and multispecialty […] The post Episode 95. “You're Breaking my Heart”: Acute Coronary Syndrome appeared first on The Pharm So Hard Podcast.
© 2020-2026 Ivy Podcast Discovery LLC
