
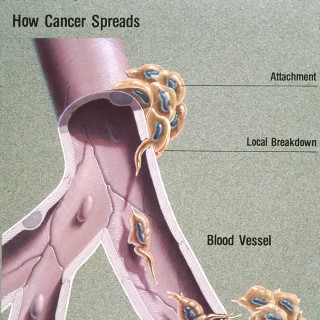
Spread of a disease inside a body
POPULARITY
Categories

368 episodes with metastatic

58 episodes with metastatic

123 episodes with metastatic

39 episodes with metastatic

21 episodes with metastatic

19 episodes with metastatic

26 episodes with metastatic

23 episodes with metastatic

33 episodes with metastatic

32 episodes with metastatic

31 episodes with metastatic

17 episodes with metastatic

19 episodes with metastatic

16 episodes with metastatic

15 episodes with metastatic

13 episodes with metastatic

22 episodes with metastatic

13 episodes with metastatic

13 episodes with metastatic

10 episodes with metastatic

13 episodes with metastatic

8 episodes with metastatic

12 episodes with metastatic

11 episodes with metastatic

12 episodes with metastatic

13 episodes with metastatic

14 episodes with metastatic

10 episodes with metastatic

8 episodes with metastatic

21 episodes with metastatic

9 episodes with metastatic

13 episodes with metastatic

10 episodes with metastatic

11 episodes with metastatic

17 episodes with metastatic

6 episodes with metastatic

9 episodes with metastatic

9 episodes with metastatic

9 episodes with metastatic

5 episodes with metastatic

9 episodes with metastatic

10 episodes with metastatic

9 episodes with metastatic

10 episodes with metastatic

12 episodes with metastatic

10 episodes with metastatic

3 episodes with metastatic

11 episodes with metastatic

5 episodes with metastatic

5 episodes with metastatic

6 episodes with metastatic

6 episodes with metastatic

8 episodes with metastatic

5 episodes with metastatic
Welcome to the Komen Health Equity Revolution series on Real Pink — where patients, advocates, researchers and community partners come together to talk honestly about what's standing in the way of breast health equity, and what we're doing to change it. June is Pride Month — a time to celebrate identity, community and the courage it takes to live authentically. Today's conversation sits right at the heart of that. Because advocating for yourself, knowing your body and refusing to be dismissed, that's not just a health message. That's a love letter to who you are. Our guest today is Shelby Smith. She was 30 years old when she noticed something felt off. No family history of breast cancer. Young, healthy, going about her life as a wife and mom to a 7-year-old daughter. But she trusted herself — and that decision changed everything. Shelby faced a 12-centimeter tumor, a bilateral mastectomy, 16 rounds of chemo and 15 rounds of radiation. She did her own research, built her own notebook, asked her own questions — and came out the other side with a message she wants every young woman to hear: Know your normal. And when something doesn't feel right, advocate for yourself. Key Takeaways: Trust your instincts when something feels off Self-advocacy can change outcomes Being informed helps patients navigate treatment Cancer can affect more than physical health Including loved ones in the journey matters Chapters 00:00 Introduction: Shelby's Breast Cancer Story 02:07 Discovering a Lump and Seeking Answers 04:37 Diagnosis, Testing, and Receiving the News 10:07 Research, Self-Advocacy, and Navigating Treatment 17:33 Identity, Family, and Talking to Her Daughter 24:46 Life After Treatment and Advice for Young Women Learn more at realpink.komen.org and komen.org Real Pink, by Susan G. Komen, shares real stories and expert insights to support people navigating breast cancer, from diagnosis through survivorship.
AUA2026: Focus on: Metastatic Urothelial Carcinoma CME Available: https://cme.auanet.org/URL/FOCUS264ONL LEARNING OBJECTIVES: After participating in this CME activity, participants will be able to: 1. Select appropriate first-line therapies for patients with locally advanced or metastatic urothelial carcinoma during initial treatment planning, in accordance with updated NCCN guidelines. 2. Evaluate holistic management approaches, including treatment sequencing, therapy transitions, and long-term follow-up for patients with locally advanced or metastatic urothelial carcinoma throughout the course of disease. 3. Implement strategies to recognize, monitor, and mitigate treatment-related adverse events in patients receiving systemic therapy for locally advanced or metastatic urothelial carcinoma. 4. Integrate shared decision-making tools and communication strategies into clinical practice to ensure alignment of treatment choices with patient values and caregiver input. 5. Distinguish between treatment pathways for different stages of advanced bladder cancer, including variant histologies to ensure accurate staging and appropriate therapy selection based on the latest NCCN guidelines. ACKNOWLEDGEMENTS Support provided by independent educational grants from: Merck & Co., Inc. Pfizer, Inc.
A breast cancer diagnosis may feel like it changes your entire life in an instant, but it doesn't get to define who you are or make all your choices for you. On today's episode of Real Pink, we're joined by Amanda Sangemino, a remarkable young woman whose diagnosis came at an age when cancer was likely the last thing on her mind. What began with a concern that was initially dismissed ultimately led her to trust her instincts, advocate for herself, and make a series of personal decisions about her treatment and future. Throughout the process, she was determined not to let fear and cancer make every decision for her. Today, she'll talk about the choices that she made about fertility, surgical options and maintaining an active lifestyle and why trusting yourself can be one of the most powerful tools you have. Key Takeaways: Mindset can play a powerful role during treatment Trust your instincts and advocate for yourself Maintaining normalcy can be empowering Don't let cancer make every decision for you A strong support system makes a difference Chapters: 00:00 – Amanda's Breast Cancer Story Begins 01:28 – Finding a Lump and Receiving a Misdiagnosis 04:22 – Seeking a Second Opinion and Getting Answers 07:00 – Why Self-Advocacy Matters for Young Women 10:00 – Fertility, Menopause, and Treatment Decisions 14:43 – Choosing Surgery, Staying Active, and Building Support 23:09 – Amanda's Final Advice Learn more at realpink.komen.org and komen.org Real Pink, by Susan G. Komen, shares real stories and expert insights to support people navigating breast cancer, from diagnosis through survivorship.

Can you really treat prostate cancer effectively without knowing the genetics? In this episode of BackTable Urology, Dr. Evan Yu and Dr. Tanya Dorff join host Dr. Alan Tan to discuss why genetic testing is essential in personalized prostate cancer care. They discuss when and how to perform germline and somatic testing, address common barriers, and share best practices for counseling patients. --- Get the BackTable apphttps://www.backtable.com/app --- This podcast is supported by an educational grant from Pfizer. --- Timestamps 00:00 - Introduction02:18 - Who Gets Somatic Testing?06:43 - Patient Barriers to Testing09:00 - Genetic Testing Workflow12:28 - Treating BRCA2 Alterations24:18 - Monitoring Progression: ctDNA vs. PSA vs. Imaging29:32 - Treating mCRPC with ATM Mutations34:39 - CDK12 Classification 37:43 - Closing Takeaways --- More about this episode The doctors explore how BRCA2 and other DNA repair alterations can directly shape treatment decisions, focusing on the roles of PARP inhibitors and platinum therapy in advanced cases. The discussion highlights why both germline and somatic testing are critical for identifying actionable mutations and discuss the nuances of interpreting test results, including current limitations and emerging biomarkers. They also examine challenges such as insurance coverage, patient misconceptions, and workflow integration, as well as the movement toward truly personalized, biology-driven approaches in prostate cancer care. --- Resources Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: a randomized phase 3 trial:https://pmc.ncbi.nlm.nih.gov/articles/PMC12705445/ Capivasertib plus abiraterone in PTEN-deficient metastatic hormone-sensitive prostate cancer: CAPItello-281 phase III study:https://www.annalsofoncology.org/article/S0923-7534(25)04936-1/fulltext Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer:https://www.nejm.org/doi/full/10.1056/NEJMoa1903307 ARCHES 5-year Survival with Enzalutamide Plus Androgen-deprivation Therapy in Metastatic Hormone-sensitive Prostate Cancer Patientshttps://www.sciencedirect.com/science/article/pii/S0302283825048766 First-Line Camizestrant for Emerging ESR1-Mutated Advanced Breast Cancer:https://www.nejm.org/doi/abs/10.1056/NEJMoa2502929 PROMISE Registry:https://www.prostatecancerpromise.org/ Talazoparib plus enzalutamide in men with HRR-deficient metastatic castration-resistant prostate cancer: final overall survival results from the randomised, placebo-controlled, phase 3 TALAPRO-2 trial:https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)00683-X/abstract --- BackTable Urology is the go-to podcast for urologists, urologic oncologists, and urogynecologists. Download the free BackTable app to get early access to new episodes, cases, and courses curated by physicians in your specialty. ► https://www.backtable.com/app
In this episode of the Oncology Brothers podcast, we discussed challenging cases focused on metastatic non-small cell lung cancer (NSCLC) with common EGFR mutations. Joined by experts Dr. Shirish Gadgeel from the Emory University and Dr. Wade Iams from Tennessee Oncology, the discussion revolved around two real-life patient cases. The first case featured a 54-year-old gentleman with active tobacco use and diffusely metastatic NSCLC, including an isolated brain lesion. The panel explored treatment options, including single-agent osimertinib versus dual combinations of amivantamab-lazertinib and osimertinib-chemotherapy, emphasizing the importance of shared decision-making and considering co-mutations and patient demographics. In the second case, the conversation shifted to supportive care and managing side effects, particularly focusing on skin toxicity associated with amivantamab. The experts shared their proactive approaches to patient education and the significance of monitoring and adjusting treatment plans to enhance patient quality of life. Key Points: In EGFR-mutated NSCLC with CNS metastases, treatment selection between single-agent osimertinib and combination amivantamab-lazertinib vs. osimertinib-chemotherapy requires individualized consideration of age, co-mutations, extent of disease, and patient preference rather than mutation status alone. Younger patients with CNS disease may benefit from more aggressive upfront combination therapy, while shared decision-making remains central to navigating the expanded efficacy versus increased toxicity trade-off. Dermatologic toxicities associated with amivantamab requires proactive management including supportive care regimen, early dose adjustments and close patient monitoring to maintain treatment continuity. Providing the best available upfront therapy in metastatic EGFR-mutated NSCLC is critical, as sequencing options become more limited at progression. Join us for an insightful discussion on the latest treatment algorithms, the importance of personalized care, and the evolving landscape of NSCLC management. Listen us on: Spotify: https://open.spotify.com/show/31BXhY9FM4gPWG10WgE11o Apple Podcast: https://podcasts.apple.com/us/podcast/oncology-brothers-practice-changing-cancer-discussions/id1653340966 Follow us on social media: X/Twitter: https://twitter.com/oncbrothers Instagram: https://www.instagram.com/oncbrothers Website: https://oncbrothers.com/ Don't forget to subscribe for more episodes featuring conference highlights and challenging cases in oncology! #EGFRMutated, #LungCancer, #ThoracicOncology, #PersonalizedMedicine, #OncologyBrothers
Today on National Cancer Survivor's Day, we're joined by a remarkable performer whose strength, vulnerability, and resilience have inspired millions around the world. She has taken the stage as a backup vocalist for numerous top artists and most recently dazzled the crowds on the biggest tour in music history with global superstar Taylor Swift. However, audiences were moved even more deeply when she chose to publicly share something far more personal – her breast cancer journey. After Jeslyn Gorman's diagnosis become known through The Eras Tour docuseries, fans witnessed the emotional reality of navigating cancer while stepping away from a career and community she loves so deeply. From continuing to tour in the early days of diagnosis, to facing treatment side effects and returning to the stage immediately following treatment, her story is one of courage, grace and resilience. Today, Jeslyn opens up about the support she received, what survivorship looks like now and most importantly, shares an empowering message for young women about listening to their bodies, advocating for their health, and never underestimating the importance of early detection. Key Takeaways: Early detection can save lives. You can experience joy and fear at the same time. A strong support system makes a major difference. Recovery is gradual and requires patience. Cancer changes your life, but it doesn't define it. Chapters 00:00 – Jeslyn's Breast Cancer Diagnosis 05:24 – Continuing to Perform After Diagnosis 07:38 – Going Public With Her Cancer Story 13:22 – Breast Health and Self-Advocacy 18:07 – Support From Family, Friends, and the Tour Community 22:17 – Staying Positive During Treatment 25:17 – Chemotherapy and Physical Recovery 31:49 – Hair Loss and Identity Learn more at realpink.komen.org and komen.org Real Pink, by Susan G. Komen, shares real stories and expert insights to support people navigating breast cancer, from diagnosis through survivorship. 37:29 – Life After Treatment and Survivorship
This episode tells the story of how one man, Jake Messier, who is living with metastatic male breast cancer, is challenging the stigma surrounding this disease, which affects 1% of all breast cancer patients. It's an important reminder that not all cancers are funded and researched equally, and that behind every statistic is a person trying to live a normal life.Jake has used his lifelong PR skills to turn what is a diagnosis unlike any other into a conversation about equity, resilience and a deep societal stigma. This conversation should also serve as a reminder of how patients perceive the healthcare system and that communication is key when treating patients, many of whom are vulnerable.A huge thank you to Jake for coming on the show. If you want more information, see Jake's website: https://www.theguywithstage4breastcancer.com/For more episodes, resources and blog posts, visit www.inquisitiveonc.comPlease find us on Twitter @InquisitiveOnc!If you want us to look at a specific trial or subject, email us at inquisitiveonc@gmail.comArt courtesy of Taryn SilverMusic courtesy of AlisiaBeats: https://pixabay.com/users/alisiabeats-39461785/Disclaimer: This podcast is for educational purposes only. If you are unwell, seek medical advice.Oncology for the Inquisitive Mind is recorded with the support of education grants from our foundation partners Pfizer and Merck Pharmaceuticals. Our partners have access to the episode at the same time you do and have no editorial control over the content. Hosted on Acast. See acast.com/privacy for more information.

Has America abandoned the values that once shaped Western civilization? In this episode of 1819 News: The Podcast, host Bryan Dawson examines Pride Month, the rise of what he calls "Christless Conservatism," and the cultural forces he believes have transformed America over the last several decades. Bryan discusses the sexual revolution, the role of modern conservatism, the decline of traditional family values, and why he believes the Christian family remains the foundation of a healthy society. He also explains why many conservatives failed to resist cultural change and what Christians can do to reclaim their influence in the public square. Topics include: • Pride Month and modern cultural politics • The rise of Christless Conservatism • Faith, family, and Western civilization • The sexual revolution and its consequences • Christian responsibility in the culture war • Building strong families in a changing America Subscribe to 1819 News for more conversations on faith, culture, politics, and the issues shaping Alabama and the nation.

Has America abandoned the values that once shaped Western civilization? In this episode of 1819 News: The Podcast, host Bryan Dawson examines Pride Month, the rise of what he calls "Christless Conservatism," and the cultural forces he believes have transformed America over the last several decades. Bryan discusses the sexual revolution, the role of modern conservatism, the decline of traditional family values, and why he believes the Christian family remains the foundation of a healthy society. He also explains why many conservatives failed to resist cultural change and what Christians can do to reclaim their influence in the public square. Topics include: • Pride Month and modern cultural politics • The rise of Christless Conservatism • Faith, family, and Western civilization • The sexual revolution and its consequences • Christian responsibility in the culture war • Building strong families in a changing America Subscribe to 1819 News for more conversations on faith, culture, politics, and the issues shaping Alabama and the nation.
As part of the 2026 UCSF Patient Conference on Prostate Cancer, Dr. Arpita Desai discusses metastatic hormone sensitive prostate cancer. Series: "Prostate Cancer Patient Conference" [Health and Medicine] [Show ID: 41560]
As part of the 2026 UCSF Patient Conference on Prostate Cancer, Dr. Arpita Desai discusses metastatic hormone sensitive prostate cancer. Series: "Prostate Cancer Patient Conference" [Health and Medicine] [Show ID: 41560]
As part of the 2026 UCSF Patient Conference on Prostate Cancer, Dr. Arpita Desai discusses metastatic hormone sensitive prostate cancer. Series: "Prostate Cancer Patient Conference" [Health and Medicine] [Show ID: 41560]
This episode originally aired in November 2023. When someone has metastatic breast cancer, it is scary for them - and for you! What can you do to really help? What should you say? Is it better to just listen? Today's guest received a de novo metastatic diagnosis in January 2021 and then elected to retire early from a 30-year technology sales career in order to slow life down and to focus on family, friends and thriving with MBC. Carlee Dixon's surprise diagnosis also inspired her to learn as much as possible about breast cancer and take every opportunity to educate friends and acquaintances about breast cancer prevention and the day to day reality. Today, Carlee is here to shed some light on how to best support those who are living with metastatic breast cancer.

In this JCO PO Article Insights episode, host Jordan Goldstein summarizes the article, "EXONERATE-TRaCE: A Liquid Biopsy for Tracking Response to Anti–Epidermal Growth Factor Receptor–Based Therapy in Metastatic Colorectal Cancer" byTakahashi, et al. LINK TO FULL TRANSCRIPT
Trisha Wise-Draper, MD, PhD - Beyond the Virus: New Strategies to Improve Outcomes of Non-HPV-Associated Recurrent/Metastatic Head and Neck Cancer
Marwan Fakih, MD - Making a Difference in Refractory Metastatic Colorectal Cancer: Practical Strategies to Positively Impact the Patient Journey Across Practice Settings
Trisha Wise-Draper, MD, PhD - Beyond the Virus: New Strategies to Improve Outcomes of Non-HPV-Associated Recurrent/Metastatic Head and Neck Cancer
Marwan Fakih, MD - Making a Difference in Refractory Metastatic Colorectal Cancer: Practical Strategies to Positively Impact the Patient Journey Across Practice Settings
Trisha Wise-Draper, MD, PhD - Beyond the Virus: New Strategies to Improve Outcomes of Non-HPV-Associated Recurrent/Metastatic Head and Neck Cancer
Trisha Wise-Draper, MD, PhD - Beyond the Virus: New Strategies to Improve Outcomes of Non-HPV-Associated Recurrent/Metastatic Head and Neck Cancer
It's Women's Health Month — which means a lot of awareness messaging and a lot of conversation about why women's health matters. But today, we're going a level deeper. Because awareness doesn't save lives. Action does. Infrastructure does. Investment does. And honest conversations about why the system isn't working equally for everyone — those matter too. My guest today is Jenica Patterson — a neuroscientist turned health systems architect who is doing the hard work of figuring out why women's health is so chronically underinvested and what it will take to fix it. She leads the Women's Health Network at the Milken Institute, one of the most powerful cross-sector coalitions in this space. Before that, she built a $113 million federal program at ARPA-H (the Advanced Research Project Agency for Health) specifically designed to fast track innovation in women's health. Komen is focused on breast health access — and the sobering reality that where you live and what you look like still determine whether you get a timely mammogram, an accurate diagnosis or the best possible care. Jenica has the research, the relationships and the conviction to tell us exactly why that is — and what's possible. Key Takeaways: Women's health inequities are systemic, not individual. Nearly 30% of U.S. counties do not have a mammography machine. Women's health has historically been underrepresented in research and clinical development. Innovation alone is not enough without integration. Momentum in women's health is growing. Chapters 00:00 Jenica Patterson's journey from neuroscience to women's health systems leadership 05:45 Why women's health is at a major inflection point 08:40 The shocking mammography access gaps across the United States 14:02 Why solving women's health requires system-wide integration 20:03 Where momentum and hope are growing in women's health equity Learn more at realpink.komen.org and komen.org breastcancer #survivorship #womenshealth #cancersupport #realpink Real Pink, by Susan G. Komen, shares real stories and expert insights to support people navigating breast cancer, from diagnosis through survivorship.
Menopause – it may be the most unwanted time in a woman's life. It arrives with a vengeance, forcing all kinds of emotional, hormonal and bodily changes onto women as they approach their 50s. But for women going through breast cancer treatment, it can arrive even earlier and be even more unwanted. The good news is no one has to suffer in silence. Today's guests are Dr. Makeba Williams, the incoming president of The Menopause Society, and Claudia McConnell, a breast cancer survivor who was forced into menopause during breast cancer treatment at age 37. Key takeaways Breast cancer treatment can trigger sudden and emotionally overwhelming early menopause Menopause symptoms after cancer treatment are real, serious, and treatable. Mental health support is a critical part of breast cancer survivorship care. Open conversations help reduce stigma and empower women to seek support. Chapters 00:00 Introduction to breast cancer and menopause realities 04:29 Claudia's breast cancer diagnosis and sudden menopause at 37 15:42 Why survivors shouldn't suffer through menopause symptoms alone 19:20 New menopause treatments and advances for breast cancer survivors 21:07 Sleep disruption, insomnia, and menopause management strategies 24:07 Estrogen creams, vaginal health, and treatment decision-making 30:19 BRCA2, talking to children about cancer risk, and family support 39:05 Final advice for women navigating menopause after breast cancer Learn more at realpink.komen.org and komen.org breastcancer #menopause #survivorship #womenshealth #cancersupport #realpink Real Pink, by Susan G. Komen, shares real stories and expert insights to support people navigating breast cancer, from diagnosis through survivorship.
Featuring an interview with Dr Wassim Abida, including the following topics: Comparing the clinical relevance of BRCA1 and BRCA2 mutations in prostate cancer (0:00) Relevance and interpretation of LOH (loss of heterozygosity) scores (4:37) Incidence and clinical relevance of PALB2 mutations; role of genetic counseling in the care of patients with prostate cancer (9:33) Key considerations surrounding toxicities associated with PARP inhibitors (15:25) Potential role of saruparib; evolving nomenclature in prostate cancer (22:36) Approach to newly diagnosed metastatic prostate cancer (26:16) Clinical relevance of PSMA-targeted PET imaging results (29:49) Case: A man in his mid 70s with metastatic castration-resistant prostate cancer (mCRPC) and a deleterious BRCA alteration receives olaparib/abiraterone/prednisone upon relapse (32:15) Combining PARP inhibitors with other DNA repair inhibitors; insights on the PSMAddition trial (37:14) Case: A man in his mid 60s with metastatic prostate adenocarcinoma and a BRCA germline mutation receives niraparib/abiraterone/prednisone (43:17) Case: A man in his early 60s with mCRPC and CDK12 mutations receives talazoparib/enzalutamide (45:54) CME information and select publications
Featuring a slide presentation and related discussion from Dr Wassim Abida, including the following topics: Clinical implications of homologous recombination repair gene alterations and biological rationale for the use of PARP inhibitors (0:00) Key clinical studies leading to FDA approvals of PARP inhibitors as monotherapy (5:01) Biological rationale for combining PARP inhibitors with androgen receptor pathway inhibitors and key findings from the Phase III PROpel study (11:03) Key findings from the Phase III MAGNITUDE and TALAPRO-2 studies (15:10) Summary of efficacy data with PARP inhibitors; toxicities (20:01) Key findings and conclusions from the Phase III AMPLITUDE study; future directions with PARP inhibitors (23:33) CME information and select publications

We're going to cure cancer in our lifetime." It's a rallying cry at every charity event, every fundraiser, every race. But what does that actually mean?Dr. Sonal Gandhi, a medical oncologist, joins Ditch the Labcoat to break down what most people don't understand: we already cure cancer. All the time. Early stage cancers like breast, colon, and skin cancer caught in time have cure rates approaching 90 to 100 percent.The challenge is stage four cancer. Metastatic disease. Cancer that has spread to other organs. And even there, the conversation is shifting. Cancer is increasingly becoming a chronic illness. People are living longer with it, sometimes dying with it rather than from it, just like they do with heart disease or diabetes.Dr. Gandhi walks through what "curing cancer" really means, how treatment has evolved beyond chemotherapy into targeted therapies and immunotherapy, and why prevention matters. Up to 40 percent of cancers are related to modifiable lifestyle factors: smoking, alcohol, obesity, lack of exercise. But even doing everything right doesn't guarantee you won't get cancer. Age is the number one risk factor, and we can't modify that.She also challenges the guilt people carry when they're diagnosed and reframes the fear around the "C word." Maybe it's time to pull cancer back into the middle with the menu of other chronic illnesses we manage, not cure.If you've ever wondered what "curing cancer" actually means, why some cancers are more treatable than others, or what you can do to reduce your risk, this episode will reframe how you think about one of medicine's most feared diagnoses.If you've ever wondered why so many people have unexplained symptoms, why standard treatments fail them, or what actually works when medicine runs out of answers, this episode will reframe how you see chronic illness.Dr. Sonal Gandhi's LinkedinEpisode Takeaways1. We already cure cancer. Early stage cancers (stage 1 or 2) caught in time have cure rates approaching 90 to 100 percent, depending on the type.2. Cancer is not one disease. It's dozens of diseases with different stages, treatments, and outcomes. We're better at treating some than others.3. Stage four (metastatic) cancer is increasingly becoming a chronic illness. Treatments help people live longer with cancer, sometimes dying with it rather than from it.4. Up to 40 percent of cancers are related to modifiable lifestyle factors: smoking, alcohol, obesity, and lack of exercise. Being a healthy weight matters for cancer prevention.5. Age is the number one risk factor for cancer. Every decade you get older, cells get worse at repairing mistakes. We can't modify aging.6. Only 10 to 20 percent of cancers are due to inherited genes. Most cancers happen because of the complicated interplay between lifestyle, environment, and cellular aging.7. Immunotherapy works by preventing cancer cells from turning off the immune system, but it can cause severe autoimmune side effects that need rapid treatment.8. Whole body scans and experimental blood tests sound appealing, but they often create more harm than good. Screening needs to be done in context with clear downstream action plans.Episode Timestamps03:51 – What Does "Curing Cancer" Actually Mean?08:15 – Early Stage vs. Late Stage Cancer: The Critical Difference12:42 – How Chemotherapy, Targeted Therapy, and Immunotherapy Work18:35 – Prevention: Lifestyle Factors That Reduce Cancer Risk21:50 – Why Immunotherapy Can Cause Severe Side Effects30:48 – Cancer as a Chronic Illness, Not a Death Sentence38:22 – Environmental and Occupational Cancer Risks45:51 – Why Whole Body Scans Aren't the AnswerDISCLAMER >>>>>> The Ditch Lab Coat podcast serves solely for general informational purposes and does not serve as a substitute for professional medical services such as medicine or nursing. It does not establish a doctor/patient relationship, and the use of information from the podcast or linked materials is at the user's own risk. The content does not aim to replace professional medical advice, diagnosis, or treatment, and users should promptly seek guidance from healthcare professionals for any medical conditions. >>>>>> The expressed opinions belong solely to the hosts and guests, and they do not necessarily reflect the views or opinions of the Hospitals, Clinics, Universities, or any other organization associated with the host or guests. Disclosures: Ditch The Lab Coat podcast is produced by (soundsdebatable.com) and is independent of Dr. Bonta's teaching and research roles at McMaster University, Temerty Faculty of Medicine and Queens University.
While menopause is often associated with aging, many women facing breast cancer experience it suddenly and much earlier than expected—bringing a wave of physical and emotional changes. From managing intense symptoms to confronting fears about future family-building, the journey can feel overwhelming. On today's episode, we are joined by Melody Johnson, a nurse practitioner who specializes in caring for women navigating these exact challenges. She will help us understand how treatment-induced menopause differs from natural menopause and the strategies available to cope with side effects while already carrying so much. We'll also take a closer look at fertility—an especially emotional and complex issue for younger women diagnosed before they've had the chance to start or grow their families. Whether you're newly diagnosed, supporting someone who is, or simply want to better understand this critical aspect of women's health, this conversation is here to inform, support, and remind you: you are not alone on this journey. What You'll Learn: • The difference between treatment-induced and age-related menopause • Common symptoms and why they can feel more severe during cancer treatment • How to manage menopause side effects alongside a breast cancer diagnosis • Fertility preservation options, including egg freezing and when to consider them • Why self-advocacy is critical when discussing fertility with your care team Chapters: 00:00 Introduction to treatment-induced menopause 01:29 Melody Johnson's background in oncofertility 02:45 What to expect from menopause symptoms 05:05 Key differences between induced and natural menopause 06:24 Managing symptoms during treatment 08:29 Fertility concerns for younger women 10:25 Is treatment-induced menopause permanent? 11:53 Questions to ask your doctor 13:24 Why these conversations matter 14:48 Final advice for women navigating fertility after diagnosis Learn more at komen.org and realpink.komen.org BreastCancer #Fertility #Menopause #WomensHealth #Oncofertility #CancerSupport #ReproductiveHealth #RealPink Real Pink, by Susan G. Komen, shares real stories and expert insights to support people navigating breast cancer, from diagnosis through survivorship.
Welcome to the Oncology Brothers podcast! In this episode, we dived deep into the exciting world of metastatic non-small cell lung cancer (NSCLC) with a focus on targeted mutations in the frontline setting. Listen us on: Spotify: https://open.spotify.com/show/31BXhY9FM4gPWG10WgE11o Apple Podcast: https://podcasts.apple.com/us/podcast/oncology-brothers-practice-changing-cancer-discussions/id1653340966 Follow us on social media: X/Twitter: https://twitter.com/oncbrothers Instagram: https://www.instagram.com/oncbrothers Website: https://oncbrothers.com/ We were joined by Dr. Eric Singhi from MD Anderson Cancer Center, to discuss the latest advancements in treatment options, including: Common EGFR mutations and the benefits of combination therapies over single-agent osimertinib. The role of CNS involvement in treatment decisions and the importance of patient-centered care. Strategies for managing disease progression and the significance of re-biopsy. Insights into ALK-positive disease, including the efficacy of lorlatinib and alectinib. The latest developments in treating rare mutations like NTRK, MET, RET, and HER2. With a wealth of clinical data and practical insights, this episode is packed with valuable information for oncologists and healthcare professionals. Tune in to learn how to navigate the complexities of NSCLC treatment and improve patient outcomes. Don't forget to subscribe for more discussions on oncology topics and share your thoughts in the comments below! #LungCancer, #TargetedTherapy, #PrecisionMedicine, #NGS, #OncologyBrothers
Welcome to the Oncology Brothers podcast! In this episode, we dived deep into the treatment algorithm for metastatic non-small cell lung cancer (NSCLC) without actionable driver mutations in frontline settings. Listen us on: Spotify: https://open.spotify.com/show/31BXhY9FM4gPWG10WgE11o Apple Podcast: https://podcasts.apple.com/us/podcast/oncology-brothers-practice-changing-cancer-discussions/id1653340966 Follow us on social media: X/Twitter: https://twitter.com/oncbrothers Instagram: https://www.instagram.com/oncbrothers Website: https://oncbrothers.com/ We discussed the latest updates in lung cancer treatment, including the recent approval of Teliso-V for C-MET overexpressing disease and Zongertinib for HER2 positive cases. We explored the nuances of choosing between single-agent and dual checkpoint inhibitors, the role of PD-L1 scores, and the impact of molecular testing on treatment decisions. Special guest Dr. Christine Garcia, a thoracic medical oncologist and fellowship program director at Weill Cornell Medicine, shared her insights on the importance of biomarker testing, the implications of STK11 and KEAP1 mutations, and the evolving landscape of KRAS inhibitors. Key topics covered in this episode: The significance of NGS testing and PD-L1 scores in treatment decisions The role of chemotherapy in high PD-L1 patients Insights on dual checkpoint inhibitors based on recent clinical trials The latest options for KRAS G12C mutations and C-MET overexpression Practical considerations for managing treatment-related side effects Tune in for an informative discussion that bridges the gap between academic research and community practice in oncology. Don't forget to subscribe for more episodes on treatment algorithms and the latest in cancer care! #MetastaticNSCLC, #Immunotherapy, #KRASG12C, #BiomarkerTesting, #OncologyBrothers
Today's conversation is one that so many mothers will feel deep in their bones because it talks about what happens when life asks you to be the one who needs care. Our guest today has lived that shift in a profound way. In the midst of raising her young children, navigating the everyday chaos and fiercely advocating for her youngest daughter, Nylah, who was born with congenital heart disease, Nisha Jaime was suddenly diagnosed with breast cancer. There is an emotional whiplash to being the strong one for your child and then suddenly needing that same strength for yourself. Nisha will talk to us about what that was like and how she balanced it all with the help of her village. We'll talk about the ongoing realities of survivorship, including things like scanxiety and continued care and how her children are involved in her journey. Most importantly, we'll hear how she has turned her experience into support for other mothers walking a similar path and why that mission matters so deeply to her.
Two Onc Docs, hosted by Samantha A. Armstrong, MD, and Karine Tawagi, MD, is a podcast dedicated to providing current and future oncologists and hematologists with the knowledge they need to ace their boards and deliver quality patient care. Dr Armstrong is a hematologist/oncologist and assistant professor of clinical medicine at Indiana University Health in Indianapolis. Dr Tawagi is a hematologist/oncologist and assistant professor of clinical medicine at the University of Illinois in Chicago.In this episode, OncLive On Air® partnered with Two Onc Docs to provide a comprehensive review of metastatic urothelial carcinoma management, contrasting historical standards with the rapidly evolving frontline paradigm. As the field transitions into a new era of care, Drs Armstrong and Tawagi emphasized the importance of understanding trial data and toxicity management for both board preparation and clinical practice.The discussion began with details about the historical treatment paradigm, which relied on platinum-based chemotherapy followed by maintenance avelumab for patients who did not progress. However, the experts noted that the current SOC has shifted dramatically following findings from the landmark EV-302 trial, which evaluated the combination of enfortumab vedotin and pembrolizumab.They also explained that the toxicities associated with enfortumab vedotin plus pembrolizumab are highly testable and clinically relevant. Key adverse effects include skin toxicity and peripheral neuropathy, they said. Additionally, the hosts highlighted hyperglycemia and the risk of diabetic ketoacidosis, and emphasized that ocular toxicities, specifically dry eyes, also necessitate referrals to ophthalmology.In the second-line setting following enfortumab vedotin plus pembrolizumab, Drs Armstrong and Tawagi noted that the paradigm unclear, though treatment options include platinum-based chemotherapy or targeted agents. They recommended testing for FGFR mutations to determine patient eligibility for erdafitinib, as well as testing for HER2 expression to determine eligibility for trastuzumab deruxtecan.They also reported that for localized high-grade upper tract urothelial carcinoma, treatment options include neoadjuvant split-dose gemcitabine/cisplatin or upfront surgery followed by adjuvant chemotherapy. In the metastatic setting, they noted that rare disease variants like small cell carcinoma are treated with platinum doublets and immunotherapy, whereas adenocarcinoma management may require FOLFOX.
Today's episode is focusing on what you need to know regarding metastatic bladder cancer, with 2026 updates. This will include the need to know treatment options and toxicities for metastatic urothelial carcinoma, and also discuss the management of upper tract + variant non-urothelial histology.
In a conversation with CancerNetwork®, Diane Simeone, MD, discussed the implications of daraxonrasib demonstrating meaningful improvements in survival among patients with metastatic pancreatic ductal adenocarcinoma (PDAC) in the phase 3 RASolute 302 trial (NCT06625320). Topline findings from the trial showed that the novel multiselective RAS(ON) inhibitor approximately doubled the median overall survival (OS) compared with investigator's choice of chemotherapy, with survival benefits extending to those with different RAS mutations and RAS wild-type disease.Simeone spoke about the significance of these results in the context of the pancreatic cancer field, breaking down how daraxonrasib's mechanism of action as a pan-RAS inhibitor may open a “new fronter” beyond standard-of-care chemotherapy and platinum-based regimens. She also touched upon the prominent toxicities that have emerged with daraxonrasib, including rashes, while emphasizing the balancing of risk and benefit as part of further optimizing RAS therapeutics.The discussion also highlighted strategies for expanding genetic testing for patients with pancreatic cancer, as Simeone described the importance of receiving second opinions at comprehensive cancer centers where multidisciplinary teams can guide patients towards personalized treatment plans. She also mentioned how initiatives such as the Pancreatic Cancer Early Detection (PRECEDE) Consortium represent viable opportunities for continuing to elevate the quality of care for patients.“This has been a Holy Grail type of thing, where people have been wanting to target KRAS but it's been a challenge. This has been a breakthrough,” Simeone said regarding the results seen with daraxonrasib. “While the effect is dramatic in patients with metastatic cancer—and unfortunately that's still half of patients who walk in the door with pancreatic cancer—applying this therapy to stage I cancer could be even more profound and drive cures. Investment in early detection, partnered with these advances in therapeutics, is where we will see the most significant progress in increasing survival rates.”Simeone is the director of the Moores Cancer Center at University of California San Diego Health.ReferenceDaraxonrasib demonstrates unprecedented overall survival benefit in pivotal phase 3 RASolute 302 clinical trial in patients with metastatic pancreatic cancer. News release. Revolution Medicines. April 13, 2026. Accessed April 29, 2026. https://tinyurl.com/44t5vh5d
Good therapeutic options for metastatic colorectal cancer are limited after the fluoropyrimidine-based options are exhausted. This week, we explore the role of trifluridine-tipiracil (Lonsurf) and bevacizumab (VEGF inhibitor), and a newish kid on the block, fruquitinib, an oral tyrosine kinase inhibitor and vascular endothelial growth factor receptor. While not perfect, they do represent later-line options for patientsStudies discussed in this episode:SUNLIGHTFRESCO-2 For more episodes, resources and blog posts, visit www.inquisitiveonc.comPlease find us on Twitter @InquisitiveOnc!If you want us to look at a specific trial or subject, email us at inquisitiveonc@gmail.comArt courtesy of Taryn SilverMusic courtesy of AlisiaBeats: https://pixabay.com/users/alisiabeats-39461785/Disclaimer: This podcast is for educational purposes only. If you are unwell, seek medical advice.Oncology for the Inquisitive Mind is recorded with the support of education grants from our foundation partners Pfizer and Merck Pharmaceuticals. Our partners have access to the episode at the same time you do and have no editorial control over the content. Hosted on Acast. See acast.com/privacy for more information.


Daraxonrasib, a first-in-class oral RAS inhibitor, nearly doubled overall survival versus chemotherapy in previously treated metastatic pancreatic cancer, representing a potentially landmark advance in a historically difficult-to-treat disease. The antibody-drug conjugate datopotamab deruxtecan significantly improved progression-free and overall survival over chemotherapy in first-line triple-negative breast cancer, particularly for patients ineligible for immunotherapy. A Cochrane review of nearly 20,000 patients found anti-amyloid Alzheimer's therapies offer minimal clinically meaningful cognitive benefit while carrying meaningful safety risks, complicating their real-world use.
What does it take to turn the most terrifying moment of your life into a movement? For Yvonne McLean Florence, it started with discovering a lump she acted on right away. Yvonne is a HER2-positive breast cancer survivor, ordained minister, Worship in Pink Ambassador, former founder of Sisters R Us Circle of Survivors (SRUCOS) and is currently the reigning Ms. Pennsylvania Senior America 2025. But before all of that, she was a wife, a mother, a grandmother — and suddenly, a patient. In this powerful episode of Real Pink, Yvonne joins host Adam Walker to talk about what it felt like to receive a life-changing diagnosis, how her faith in God, family and friends carried her through chemotherapy and Herceptin infusions, and why she didn't stop when treatment ended. She'll share how she's bringing the conversation about breast health into churches across Philadelphia through Worship in Pink, what it means to build a Cancer Survivorship Resource Nook inside a congregation, and why she would like every survivor to discover how they can also reach back. This episode is part of our Health Equity Revolution series, which lifts up the voices, stories and solutions of the communities most impacted by breast cancer disparities.
Host Jake New summarizes and offers insights into the JCO article by Licitra et al., "Pembrolizumab With or Without Lenvatinib as First-Line Therapy for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: Phase III LEAP-010 Study." LINK TO FULL TRANSCRIPT

Join Dr. Martin in today's episode of The Doctor Is In Podcast.
OsteoBites welcomes Caroline Maloney, MD, PhD, from the Medical College of Wisconsin, who will discuss her research on surgery-accelerated metastasis and developing perioperative therapies.Pulmonary metastasis remains the major cause of death in osteosarcoma. The timing of metastatic relapse defines clinically meaningful subgroups in osteosarcoma with patients who relapse within 6–12 months of surgical removal of their primary tumor having markedly worse survival (10-20%) than those who relapse after completion of therapy (40-50%). While surgical removal of the primary tumor is a fundamental component of the clinical care of solid tumors, surgery induces transient but profound changes in immune and inflammatory responses that can paradoxically accelerate the growth of metastatic disease. Dr. Maloney has demonstrated that surgical removal of the primary tumor accelerates the growth of pre-existing pulmonary metastatic disease and promotes expansion of M2‐like macrophages in the lung microenvironment. Strikingly, short term perioperative treatment with a RIPK2 inhibitor blocks this effect and reprograms macrophages toward an M1-like phenotype, implicating the NOD2–RIPK2 innate immune pathway as a key mediator of post‐surgical immune reprogramming. In contrast, the NOD2 agonist Mifamurtide has shown clinical efficacy when administered as adjuvant therapy to metastatic osteosarcoma patients after primary tumor resection. This data suggests that NOD/RIPK2 signaling may exert context-dependent effects, promoting either pro- or anti-tumor myeloid responses depending on the timing of activation relative to surgery. Understanding how surgical tumor removal alters systemic innate immunity and how RIPK2 signaling orchestrates these responses could identify new strategies to prevent early pulmonary relapse after surgery.
People who had radiation treatment to the chest area for certain types of cancer early in life have an increased risk of breast cancer later in life. Today, we welcome a special guest back to the show, Amy Colver. Amy is Manager of Health Information & Publications at Komen and an oncology certified, licensed independent social worker who has worked in the oncology space, so she knows more about cancer from an educational standpoint than most. Today, she is here to share that she's also a cancer survivor and lives with the reality that a treatment she had for lymphoma in young adulthood put her at a higher risk of breast cancer. She'll talk to us about how to process risk and what ongoing care, screening and emotional resilience really looks like. Above all, Amy knows the power of turning awareness into action, and how understanding your risk factors can become more of a source of empowerment than fear.

She was 29 years old. No family history. No warning signs. She found it herself in the shower — and it changed everything. Claire was diagnosed with breast cancer at 29, went through a lumpectomy, chemotherapy, radiation, and eight years on and off Tamoxifen — all while teaching first grade, freezing her eggs, getting married, and becoming a mom to three kids. She lived 11 and a half years of clear scans and a full, beautiful life. Then last Christmas Eve, it came back. Stage 4. Metastatic. Liver and bones. And Claire's response? "It's just a little road bump." This episode is one of the most honest, funny, and genuinely hopeful conversations about metastatic breast cancer you will ever hear. Claire is the host of Perky Bits — a blog and podcast she started in 2014 to document her journey in real time — and she holds absolutely nothing back. What we cover: Finding a golf ball-sized tumor in the shower at 29 — and what happened next How Claire worked as a first grade teacher throughout chemo and radiation Why she froze her eggs before starting chemotherapy — and had three healthy children The GI symptoms that started in July 2024 that nobody connected to cancer for months — and the critical warning signs metastatic survivors need to know Getting the call on Christmas Eve that it had spread to her liver and bones What it actually feels like when treatment starts working — and her tumors start shrinking How she talks to her young kids about her treatment without terrifying them The connection between stress and recurrence — and what she wishes she'd managed differently Why stage 4 is not what it used to be — and the women thriving 15+ years out The unexpected blessings cancer gave her — including the line she ends every speaking engagement with: "Thank you, cancer." Where Perky Bits came from — and the story of the older gentleman who had to hold her breast with gauze for an hour post-biopsy (you can't make this stuff up) Important message for every survivor: Claire's metastatic diagnosis showed up as GI symptoms — bloating, distension, constipation, diarrhea — not a breast lump. Your mammograms matter. But so does listening to your body everywhere else. Connect with Claire:https://www.instagram.com/claireperkybits/ Listen to Perkybits here: https://podcasts.apple.com/us/podcast/perkybits-riding-the-waves-of-life-intro/id1890866013?i=1000759385674 Connect with Jen: Community: Not Today Cancer — The Inner Circle GET BrocElite: Mara Labs supplements - Use code NotTodayCancer for 20% off Instagram: https://www.instagram.com/jendelvaux/ Email me: jen@jendelvaux.com
Featuring patient case presentations by Dr Jacqueline T Brown and Dr Nazli Dizman, with commentary from Dr Matthew Milowsky, including the following topics: Case: A woman in her early 60s with muscle-invasive bladder cancer experiences disease progression with lung metastasis after surgery and receives enfortumab vedotin (EV)/pembrolizumab (0:00) Case: A man in his mid 70s with metastatic urothelial bladder cancer (UBC) starts first-line EV/pembrolizumab with a partial response, and testing reveals HER2 IHC 3+ (10:58) Case: A man in his late 60s with progression of metastatic UBC after multiple lines of therapy for whom testing reveals HER2 IHC 3+ receives trastuzumab deruxtecan (19:18) CME information and select publications
Dr Matthew Milowsky from the UNC Lineberger Comprehensive Cancer Center in Chapel Hill, North Carolina, comments on real patient cases of metastatic urothelial bladder cancer presented by Dr Jacqueline T Brown from the Emory University School of Medicine in Atlanta, Georgia, and Dr Nazli Dizman from The University of Texas MD Anderson Cancer Center in Houston.CME information and select publications here.
Millions of women in the U.S. can access no cost screening mammograms, but if the patient is at a higher risk of breast cancer or the mammogram reveals an abnormality, the cost of imaging makes it unattainable for many. Komen has worked with state legislature to eliminate the patient's out-of-pocket costs. Unfortunately, not all states have passed such laws, and federal legislation is still pending. Susan G. Komen's Center for Public Policy is championing legislation that addresses this significant flaw in health care insurance coverage and ensuring all people have access to high-quality, affordable care. Here today to discuss Komen's public policy is Deandrea Newsome, Regional Manager of State Policy & Advocacy at Susan G. Komen. Learn more about how you can support the ABCD Act here: https://www.komen.org/how-to-help/advocacy/action-center/?vvsrc=%2fcampaigns%2f128891%2frespond%3f_gl%3d1*3b3ivi*_gcl_au*MTk3NTA1Mjk2My4xNzcwMDU5MTYy*_ga*MjUzMDUxNzk3LjE3NTYyMzI0NjI.*_ga_HGS8BJYTKQ*czE3NzU3NTExODEkbzkkZzEkdDE3NzU3NTExOTgkajQzJGwwJGgxMTE2ODQ1MzE2*_fplc*WTlIZnY0dVc3ZEpvZFZmQWElMkJpNUh6T2lNUlhTOHJWJTJGV3RyckU5OFJ0b0k5WkhJamh0RjE2c2JoVkRwbjVNcDE1SnB6d0ZnVDBTYUxhZnRwYmluZm1QSlU1bElSU05JY2ZudWZZMmd4TmxJRkROYVB6RWF1SzhNZmEwZ1FGdyUzRCUzRA..

Did you know that antibody-drug conjugates (ADCs) targeting Trop2 have demonstrated significant clinical potential for patients with TNBC? Credit available for this activity expires: 4/8/27 Earn Credit / Learning Objectives & Disclosures: https://www.medscape.org/viewarticle/front-antibody-drug-conjugates-shifting-paradigm-metastatic-2026a1000a9z?ecd=bdc_podcast_libsyn_mscpedu
We're excited today to welcome Dina Farris and her husband, Caleb, to the podcast. Dina and Caleb navigated her breast cancer diagnosis, together, one test at a time, and just weeks before their wedding. We know that breast cancer disproportionately affects the patient, but it also deeply affects the loved ones and family members who are among the biggest supporters.
We are back with a very special guest Dr. Michael Pishvaian, who is an Associate Professor in GI Oncology at the Johns Hopkins Kimmel Cancer Center, and creator of Tumor Board Tuesday. In part 2, we will focus on metastatic pancreatic cancer, 1L treatments, maintenance therapy, targeted therapy + more.
The risk of getting breast cancer increases as you get older, but breast cancer can happen at any age. Today's guest is Abby. Abby was diagnosed with Stage 3 luminal B invasive ductal carcinoma breast cancer at the young age of 31 with no prior family history. She is mom of a 4-year-old, a DIYer and spends time trying to live a more simple, happy life. This episode originally aired on May 27, 2024
AI-powered support tools are moving fast in health care — and breast cancer is no exception. In this special episode, we look at how AI companions and chat tools might expand access to support, while also raising serious concerns about accuracy, bias, privacy and inequity. Host Adam Walker is joined by breast cancer survivor Ellyn Winters-Robinson to discuss what it means to design AI with lived experience, cultural responsiveness and patient safety at the center. They explore where AI can help (navigation of information, emotional reassurance, questions to bring to appointments) and where human expertise must remain non-negotiable.

With the increasing incidence of colorectal cancer in those less than 50 years of age, one must wonder how many patients present with a Stage IV diagnosis. Take a deep dive with us discussing the management of metastatic colorectal cancer by joining our team and guests, Drs. Cathy Eng, Michael D'Angelica, and Nina Sanford.Hosts: - Dr. Janet Alvarez - General Surgery Resident at New York Medical College/Metropolitan Hospital Center- Dr. Wini Zambare – General Surgery Resident at Weill Cornell Medical Center/New York Presbyterian- Dr. Philip Bauer, Assistant Professor of Surgery, Division of Colon and Rectal Surgery, The Ohio State University Wexner Medical Center, Arthur G. James Cancer Hospital- Dr. J. Joshua Smith MD, PhD, Chair, Department of Colon and Rectal Surgery at MD Anderson Cancer Center Guest Speakers:- Dr. Michael D'Angelica MD, FACS – Hepatopancreatobiliary Surgery, Memorial Sloan Kettering Cancer Center, Enid A. Haupt Chair in Surgery, Vice Chair, Education- Dr. Cathy Eng MD, FACP - Division of Hematology and Oncology, Vanderbilt-Ingram Cancer Center, David H. Johnson Endowed Chair in Surgical and Medical Oncology, Professor of Medicine, Hematology and Oncology, VICC Associate Director for Strategic Relations and Research Partnerships, Executive Director, Young Adult Cancers Program - Dr. Nina Sanford, MD – Radiation Oncology, UT Southwestern Medical Center, Chief of Gastrointestinal Radiation Oncology Service, Associate Professor Learning Objectives:1. Review the epidemiology, prognosis, and common metastatic patterns of metastatic colorectal cancer (mCRC).2. Discuss the role of systemic chemotherapy and targeted therapies in the first- and subsequent-line treatment of mCRC, including the impact of molecular biomarkers such as MSI/MMR, RAS, BRAF, and HER2.3. Evaluate the indications and timing of surgical and locoregional therapies for metastatic colorectal cancer, particularly in patients with liver-limited or oligometastatic disease.4. Describe the multidisciplinary management of mCRC, including the roles of radiation therapy, systemic therapy sequencing, and palliative interventions to optimize outcomes and quality of life.References:Singh, M., Morris, V. K., Bandey, I. N., Hong, D. S. & Kopetz, S. Advancements in combining targeted therapy and immunotherapy for colorectal cancer. Trends Cancer 10, 598–609 (2024). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/38821852/Napolitano, S. et al. BRAFV600E mutant metastatic colorectal cancer: Current advances in personalized treatment and future perspectives. Cancer Treat. Rev. 134, (2025). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/40009904/Ciardiello, F. et al. Clinical management of metastatic colorectal cancer in the era of precision medicine. CA. Cancer J. Clin. 72, 372–401 (2022). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/35472088/Kim, S. Y. & Kim, T. W. Current challenges in the implementation of precision oncology for the management of metastatic colorectal cancer. ESMO Open 5, e000634 (2020). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/32188714/Biller, L. H. & Schrag, D. Diagnosis and Treatment of Metastatic Colorectal Cancer: A Review. JAMA 325, 669–685 (2021). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/33591350/Smith, J. J. et al. Genomic stratification beyond Ras/B-Raf in colorectal liver metastasis patients treated with hepatic arterial infusion. Cancer Med. 8, 6538–6548 (2019). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/31503397/Saadat, L. V. et al. Hepatic Artery Infusion Chemotherapy Compared to Transarterial Radioembolization For Unresectable Colorectal Liver Metastases. Ann. Surg. 10.1097/SLA.0000000000006851 doi:10.1097/SLA.0000000000006851. PubMed Link: https://pubmed.ncbi.nlm.nih.gov/?term=10.1097/SLA.0000000000006851 (Linked via DOI search as the direct PMID is still indexing)Xiao, A. & Fakih, M. KRAS G12C Inhibitors in the Treatment of Metastatic Colorectal Cancer. Clin. Colorectal Cancer 23, 199–206 (2024). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/38825433/André, T. et al. Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. N. Engl. J. Med. 383, 2207–2218 (2020). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/33264544/Morris, V. K. et al. Treatment of Metastatic Colorectal Cancer: ASCO Guideline. J. Clin. Oncol. 41, 678–700 (2023). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/36252154/Xu, Z. et al. Treatments for Stage IV Colon Cancer and Overall Survival. J. Surg. Res. 242, 47–54 (2019). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/31071604/Smith, J. J. & D'Angelica, M. I. Surgical Management of Hepatic Metastases of Colorectal Cancer. Hematol. Oncol. Clin. North Am. 29, 61–84 (2015). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/25475573/Strickler, J. H. et al. Tucatinib plus trastuzumab for chemotherapy-refractory, HER2-positive, RAS wild-type unresectable or metastatic colorectal cancer (MOUNTAINEER): a multicentre, open-label, phase 2 study. Lancet Oncol. 24, 496–508 (2023). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/37142372/Kruijssen, D. E. W. van der et al. Upfront resection versus no resection of the primary tumor in patients with synchronous metastatic colorectal cancer: the randomized phase III CAIRO4 study conducted by the Dutch Colorectal Cancer Group and the Danish Colorectal Cancer Group. Ann. Oncol. 35, 769–779 (2024). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/38852675/Hitchcock, K. E., Romesser, P. B. & Miller, E. D. Local Therapies in Advanced Colorectal Cancer. Hematol. Oncol. Clin. North Am. 36, 553–567 (2022). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/35562258/Hitchcock, K. E. et al. Alliance for clinical trials in Oncology (Alliance) trial A022101/NRG-GI009: a pragmatic randomized phase III trial evaluating total ablative therapy for patients with limited metastatic colorectal cancer: evaluating radiation, ablation, and surgery (ERASur). BMC Cancer 24, 201 (2024). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/38350888/Adam, R. et al. Liver transplantation plus chemotherapy versus chemotherapy alone in patients with permanently unresectable colorectal liver metastases (TransMet): results from a multicentre, open-label, prospective, randomised controlled trial. The Lancet 404, 1107–1118 (2024). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/39306468/Elez, E. et al. Encorafenib, Cetuximab, and mFOLFOX6 in BRAF-Mutated Colorectal Cancer. N. Engl. J. Med. 392, 2425–2437 (2025). PubMed Link: https://pubmed.ncbi.nlm.nih.gov/40444708/***Fellowship Application Link: https://forms.gle/QSUrR2GWHDZ1MmWC6Please visit https://behindtheknife.org to access other high-yield surgical education podcasts, videos and more. If you liked this episode, check out our recent episodes here: https://behindtheknife.org/listenBehind the Knife Premium:General Surgery Oral Board Review Course: https://behindtheknife.org/premium/general-surgery-oral-board-reviewTrauma Surgery Video Atlas: https://behindtheknife.org/premium/trauma-surgery-video-atlasDominate Surgery: A High-Yield Guide to Your Surgery Clerkship: https://behindtheknife.org/premium/dominate-surgery-a-high-yield-guide-to-your-surgery-clerkshipDominate Surgery for APPs: A High-Yield Guide to Your Surgery Rotation: https://behindtheknife.org/premium/dominate-surgery-for-apps-a-high-yield-guide-to-your-surgery-rotationVascular Surgery Oral Board Review Course: https://behindtheknife.org/premium/vascular-surgery-oral-board-audio-reviewColorectal Surgery Oral Board Review Course: https://behindtheknife.org/premium/colorectal-surgery-oral-board-audio-reviewSurgical Oncology Oral Board Review Course: https://behindtheknife.org/premium/surgical-oncology-oral-board-audio-reviewCardiothoracic Oral Board Review Course: https://behindtheknife.org/premium/cardiothoracic-surgery-oral-board-audio-reviewDownload our App:Apple App Store: https://apps.apple.com/us/app/behind-the-knife/id1672420049Android/Google Play: https://play.google.com/store/apps/details?id=com.btk.app&hl=en_US
© 2020-2026 Ivy Podcast Discovery LLC
