
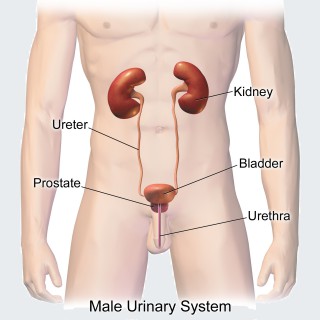
Human anatomical system consisting of the kidneys, ureters, urinary bladder, and the urethra
POPULARITY

10 episodes with urinary

6 episodes with urinary

4 episodes with urinary

6 episodes with urinary

7 episodes with urinary

3 episodes with urinary

5 episodes with urinary

5 episodes with urinary

5 episodes with urinary

3 episodes with urinary

3 episodes with urinary

3 episodes with urinary

4 episodes with urinary

3 episodes with urinary

4 episodes with urinary

4 episodes with urinary

3 episodes with urinary

4 episodes with urinary

10 episodes with urinary

3 episodes with urinary

4 episodes with urinary

2 episodes with urinary

2 episodes with urinary

3 episodes with urinary

2 episodes with urinary

3 episodes with urinary

2 episodes with urinary
Whether you're facing bladder removal surgery or supporting someone who is, choosing the right urinary diversion can feel overwhelming. In this episode, urologic oncologist Dr. Christine Ibilibor separates fact from fiction, explains the pros and cons of the different diversion options and addresses the unique concerns women often face, from body image and intimacy to recovery and quality of life. Packed with practical advice and reassuring insights, this conversation will help patients feel more informed and more confident when making one of the most important decisions in bladder cancer care.

Cameron is joined by Dr. Bushra Alzubaidi, founder of Lysty Aesthetics and Wellness, and they discuss the often-overlooked topic of women's intimate wellness. They explore the societal taboos surrounding sexual health, the impact of aging and childbirth on women's bodies, and the importance of normalizing conversations about intimate wellness. She shares her insights on the consultation process, the creation of comprehensive treatment plans, and the role of peptides in enhancing sexual wellness. The conversationCameron and Dr. Bushra emphasize the empowerment of women to speak openly about their health and the need for a supportive dialogue in the medical community. Dr. Bushra talks about the importance of women's wellness, addressing topics such as urinary incontinence, intimate wellness treatments, and the significance of patient-centric care. She emphasizes the need for open discussions about women's health issues and the evolution of treatments available. They also highlight the importance of building trust in patient-provider relationships and the connection between sexual wellness and overall happiness. Listen In!Thank you for listening to this episode of Medical Millionaire!Takeaways:Women are starting to realize they don't have to separate sexual wellness from aesthetics.Social media has played a significant role in normalizing discussions about intimate wellness.Aging and childbirth can significantly impact women's intimate health.Education is key to empowering women about their sexual wellness options.The consultation process should focus on listening to the patient's concerns first.Intimate wellness issues can affect emotional and mental well-being.Peptides can play a role in enhancing sexual wellness and libido.Women are becoming more empowered to discuss their health openly.Normalizing conversations about intimate wellness is essential for societal change.Providers need to create a safe space for women to discuss their intimate health. Women often hesitate to discuss intimate health issues due to stigma.Urinary incontinence is a common issue that can be treated effectively.Many women are unaware that treatments exist for conditions they think are normal.Patient education is crucial in intimate wellness.The market for intimate wellness is growing and evolving rapidly.Trust and authenticity in patient-provider relationships lead to better outcomes.Sexual wellness is closely linked to overall happiness and relationship stability.Men are increasingly involved in discussions about women's health.Listening to patients' experiences is essential for effective treatment.The future of wellness will focus on holistic approaches to health.Medical Millionaire: The Blueprint for Scaling a World-Class Medical Aesthetics PracticeWelcome to Medical Millionaire, the go-to podcast for forward-thinking Medspa owners, Medical Aesthetics leaders, Plastic Surgery & Dermatology practices, Concierge Wellness clinics, and Elective Healthcare entrepreneurs who are ready to scale with intention and operate like a true, high-performing business.If you're building, growing, optimizing, or preparing to exit your aesthetics or wellness practice, this show is your competitive advantage.Hosted by Cameron Hemphill Your Guide to Sustainable, Scalable Growth Your host, Cameron Hemphill, is one of the most trusted growth strategists in Medical Aesthetics and Elective Wellness.With over 10 years in the industry, Cameron has helped scale 1,000+ practices and more than 2,300 providers, working alongside the most recognized KOLs, national brands, EMRs, tech companies, and private equity groups, shaping the future of aesthetics. From marketing to operations, from finance to leadership, Cameron brings a real-world, data-driven perspective on what it takes to turn a practice into a powerful business engine.What This Podcast Is All About: Each episode takes you behind the scenes of the fastest-growing practices in the country, revealing the systems, strategies, and mindset required to win in today's Medical Aesthetics landscape.Expect tactical insights, step-by-step frameworks, and conversations with:Industry thought leadersTop injectors & medical directorsEMR & tech innovatorsOperations expertsMarketing strategistsPrivate equity & M&A advisorsWellness and longevity pioneersThis is where aesthetics, business, technology, and wellness converge. What You'll Learn on Medical Millionaire Every week, you'll access expert guidance to help you scale profitably and predictably, including:Marketing & Brand PositioningCRM + Lead Management SystemsPatient Acquisition & ConversionEMR Optimization & Tech Stack ArchitectureSales Psychology & Consultation MasteryFinance, KPIs, and Practice EconomicsOperational Workflows & AutomationIndustry Trends Backed by Real Benchmark DataPatient Retention & Lifetime Value ExpansionMindset, Leadership & Team DevelopmentWhether you're opening your first location or running a multi-million-dollar enterprise, you'll gain the clarity and direction to grow with confidence. A Show Designed for Every Stage of Practice Growth Medical Millionaire breaks down the journey into four essential stages, showing you exactly how to move from one to the next:Startup – Build the foundation and attract your first wave of patientsGrowth – Scale revenue, expand services, and strengthen operationsOptimize – Increase efficiency, margins, and customer experienceExit – Prepare your practice for maximum valuation and acquisitionIf You're Ready to Grow, This Is Where You Start. Tune in weekly for actionable insights, expert interviews, and the exact playbooks high-performing practices use to dominate their markets. This is the podcast for Medspa owners who want more than a job; they want a scalable, profitable, industry-leading business. Welcome to Medical Millionaire.Let's build your practice into the empire it deserves to be.
If you're facing bladder removal surgery, choosing a urinary diversion may be one of the most important decisions you'll ever make—and one of the hardest to understand. In this episode, reconstructive urologist Dr. Divya Ajay shares how real patient experiences inspired a first-of-its-kind decision tool that helps people compare diversion options, set realistic expectations and better prepare for life after surgery. From intimacy and travel to recovery, aging and day-to-day living, this conversation offers practical guidance that can help patients feel more informed, more confident and more in control of their treatment journey. View and download a urinary diversion decision guide.

What if one of the most important health crises affecting men today wasn't being caused by aging, but by the environment we live in? In this eye-opening solo episode, Darin Olien investigates the alarming decline in testosterone levels, fertility, and reproductive health among men worldwide. Drawing on decades of research, epidemiological studies, environmental science, endocrinology, and public health data, Darin examines the growing evidence connecting endocrine-disrupting chemicals, microplastics, sleep deprivation, chronic stress, poor lifestyle habits, and environmental toxins to declining testosterone levels across generations. From BPA, phthalates, atrazine, PFAS, and microplastics to sleep quality, circadian rhythms, cholesterol metabolism, cortisol regulation, and natural testosterone-supporting strategies, this episode explores what may be one of the most underreported public health issues of our time—and what men can do to take control of their health today. What You'll Learn Why testosterone levels have been declining for decades The startling research on global sperm count decline How endocrine-disrupting chemicals interfere with hormone production Why BPA and phthalates may disrupt testosterone synthesis The role of atrazine, PFAS, and environmental toxins How chronic stress diverts resources away from testosterone production Why sleep may be the most important testosterone intervention The connection between cholesterol and hormone production How microplastics are being found throughout the human body The surprising relationship between statins and testosterone levels Natural lifestyle strategies that support healthy hormone production Practical steps to reduce environmental exposure and improve health Chapters 00:00:00 – Welcome to SuperLife 00:00:33 – Sponsor: Fatty15 and cellular health 00:04:17 – The testosterone collapse explained 00:04:51 – Testosterone levels have been declining for decades 00:06:03 – Global sperm count decline and accelerating trends 00:07:02 – Why treating symptoms misses the root cause 00:07:27 – The hidden public health crisis 00:08:03 – Why low testosterone isn't just about aging 00:09:12 – Why hormone health affects longevity 00:09:53 – Low testosterone and increased mortality risk 00:10:35 – Testosterone's role in metabolism and cardiovascular health 00:11:27 – Endocrine-disrupting chemicals and hormone disruption 00:12:44 – BPA and its effects on testosterone production 00:13:59 – Phthalates and their impact on hormone pathways 00:16:00 – Glyphosate, atrazine, and pesticide exposure 00:17:07 – PFAS and reproductive health concerns 00:17:55 – Environmental toxins and population-wide effects 00:18:11 – Sponsor: Shakeology 00:20:02 – Cholesterol and hormone production 00:20:53 – Chronic stress and cortisol dominance 00:21:45 – Actionable solutions begin 00:21:56 – Why sleep is essential for testosterone production 00:23:07 – How sleep deprivation rapidly lowers testosterone 00:23:21 – Light pollution and circadian disruption 00:23:41 – Foods and nutrients needed for hormone health 00:24:23 – Microplastics and testicular tissue 00:24:53 – Statins and unintended hormonal consequences 00:25:39 – A practical testosterone sovereignty protocol 00:25:48 – Water filtration and reducing toxic exposure 00:26:13 – Eliminating plastics and fragrance chemicals 00:26:35 – Why organic food matters 00:26:45 – Sunlight and vitamin D 00:27:05 – Magnesium, omega-3s, and iodine 00:27:26 – Pine pollen and natural androgen support 00:28:01 – Tongkat Ali and ashwagandha 00:28:48 – Strength training and lifestyle interventions 00:29:10 – Habits that naturally support testosterone 00:29:27 – Darin's approach to healthy aging 00:29:37 – Plants, herbs, and common sense 00:29:51 – Reclaiming your health and sovereignty 00:30:00 – Final thoughts and closing message Thank You to Our Sponsors Fatty15: Get an additional 15% off their 90-day subscription Starter Kit by going to fatty15.com/DARIN and using code DARIN at checkout. Shakeology: Get 15% off with code DARINO1BODI at Shakeology.com. Join the SuperLife Patreon: This is where Darin now shares the deeper work: - weekly voice notes - ingredient trackers - wellness challenges - extended conversations - community accountability - sovereignty practices Join now for only $7.49/month at https://patreon.com/darinolien Find More from Darin Olien: Website: darinolien.com Instagram: @darinolien Book: Fatal Conveniences Platform & Products: superlife.com New Show: Roadmap to Happiness Key Takeaway "The testosterone crisis may be about far more than aging. It may be a reflection of the modern environment itself—one increasingly saturated with endocrine-disrupting chemicals, chronic stress, poor sleep, circadian disruption, and toxic exposures. While many of these forces feel outside our control, the encouraging reality is that many of the most powerful interventions remain accessible: improving sleep, reducing toxic load, eating whole foods, getting sunlight, managing stress, exercising regularly, and reclaiming responsibility for our health. The goal isn't fear. The goal is awareness—and action." Bibliography/Sources: The Decline — Primary Research Levine, H., Jørgensen, N., Martino-Andrade, A., et al. (2022). Temporal trends in sperm count: A systematic review and meta-regression analysis of samples collected globally in the 20th and 21st centuries. Human Reproduction Update, 29(2), 157–176. https://doi.org/10.1093/humupd/dmac035 Lokeshwar, S. D., Patel, P., Fantus, R. J., et al. (2021). Decline in testosterone levels in men aged 15–40: Results from the National Health and Nutrition Examination Survey (NHANES), 1999–2016. World Journal of Urology, 39(2), 447–452. https://doi.org/10.1007/s00345-020-03227-1 Spital Clinic. (2026, March). Declining testosterone levels by generation. https://www.spitalclinic.com Travison, T. G., Araujo, A. B., O'Donnell, A. B., Kupelian, V., & McKinlay, J. B. (2007). A population-level decline in serum testosterone levels in American men. The Journal of Clinical Endocrinology & Metabolism, 92(1), 196–202. https://doi.org/10.1210/jc.2006-1375 Low Testosterone — Mortality & Disease Risk Muraleedharan, V., Marsh, H., Kapoor, D., Channer, K. S., & Jones, T. H. (2013). Testosterone deficiency is associated with increased risk of mortality and testosterone replacement improves survival in men with type 2 diabetes. European Journal of Endocrinology, 169(6), 725–733. https://doi.org/10.1530/EJE-13-0321 Shores, M. M., et al. (2006). Low testosterone associated with increased all-cause and cardiovascular mortality. Archives of Internal Medicine, 166(15), 1660–1665. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/410754 Yeap, B. B., Marriott, R. J., Dwivedi, G., et al. (2024). Associations of testosterone and related hormones with all-cause and cardiovascular mortality and incident cardiovascular disease in men. Annals of Internal Medicine. https://doi.org/10.7326/M23-2781 Endocrine Disrupting Chemicals Associations between endocrine-disrupting chemical exposure and fertility outcomes: A decade of human epidemiological evidence. (2024). PubMed Central (PMC12299029). https://pmc.ncbi.nlm.nih.gov/articles/PMC12299029/ Hayes, T. B., Haston, K., Tsui, M., et al. (2002). Herbicides: Feminization of male frogs in the wild. Nature, 419, 895–896. https://doi.org/10.1038/419895a Mechanisms of testicular disruption from exposure to BPA and phthalates. (2020). Journal of Clinical Medicine, 9(2), 471. https://pmc.ncbi.nlm.nih.gov/articles/PMC7074154/ Meeker, J. D., Calafat, A. M., & Hauser, R. (2014). Urinary phthalate metabolites and their biotransformation products: Predictors and temporal variability among men and women. Journal of Exposure Science & Environmental Epidemiology. https://www.sciencedaily.com/releases/2014/08/140814124330.htm Zhao, Q., et al. (2023). Male reproductive toxicity of microplastics: Head and tail of the sperm. Science of the Total Environment, 872, 162181. https://doi.org/10.1016/j.scitotenv.2023.162181 Zhong, B., et al. (2024). Mixed EDC exposure associated with reductions in testosterone and free androgen index. Scientific Reports. https://doi.org/10.1038/s41598-024-76972-z Cortisol, Stress & the HPG Axis Bielohuby, M., et al. (2012). Swiss military cadets prolonged stress study. Psychoneuroendocrinology. Preprints.org. (2025). Sleep deprivation: A modifiable cause. https://doi.org/10.20944/preprints202505.0580.v1 SiPhox Health. (n.d.). Summary of Journal of Clinical Endocrinology & Metabolism data. https://www.siphoxhealth.com Viau, V. (2002). Functional cross-talk between the hypothalamic-pituitary-gonadal and -adrenal axes. Journal of Neuroendocrinology, 14(6), 506–513. https://doi.org/10.1046/j.1365-2826.2002.00798.x Sleep & Testosterone Leproult, R., & Van Cauter, E. (2011). Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA, 305(21), 2173–2174. https://jamanetwork.com/journals/jama/fullarticle/1029127 Reiter, R. J., et al. (2021). Melatonin and male reproductive health: Relationship to oxidative stress, mitochondrial function, and Leydig cell protection. Endocrine. Tan, D. X., Hardeland, R., Manchester, L. C., et al. (2023). Melatonin as a pleiotropic antioxidant hormone. Journal of Pineal Research. Nutrition — Zinc, Vitamin D, Cholesterol Corona, G., et al. (2010). Statin therapy and testosterone levels in men: A systematic review. The Journal of Sexual Medicine. Daniell, H. W. (2002). Hypogonadism in men consuming sustained-action oral opioids. The Journal of Pain, 3(5), 377–384. https://doi.org/10.1054/jpai.2002.126790 Pilz, S., Frisch, S., Koertke, H., et al. (2011). Effect of vitamin D supplementation on testosterone levels in men. Hormone and Metabolic Research, 43(3), 223–225. https://doi.org/10.1055/s-0030-1269854 Prasad, A. S., Mantzoros, C. S., Beck, F. W., Hess, J. W., & Brewer, G. J. (1996). Zinc status and serum testosterone levels of healthy adults. Nutrition, 12(5), 344–348. https://doi.org/10.1016/S0899-9007(96)80058-X Natural Testosterone Support — Botanical Evidence Pine pollen impacts testosterone-related symptoms in men. (2024). ACMCR Case Reports, 14(5), 1–9. Chinnappan, S. M., George, A., et al. (2021). Effect of Eurycoma longifolia standardised extract Physta on testosterone levels in ageing males: A randomised, double-blind, placebo-controlled multicentre study. Food & Nutrition Research, 65. https://doi.org/10.29219/fnr.v65.5647 Lazarev, A., & Bezuglov, E. (2021). Testosterone boosters intake in athletes: Current evidence and further directions. Endocrines, 2(2), 109–120. https://doi.org/10.3390/endocrines2020011 Leisegang, K., et al. (2022). Eurycoma longifolia (Tongkat Ali) improves serum total testosterone in men. Food & Nutrition Research. https://pubmed.ncbi.nlm.nih.gov/36013514/ Leitão, A. E., et al. (2021). 6-month double-blind RCT: Eurycoma longifolia 200mg + concurrent training. Maturitas. https://doi.org/10.1016/j.maturitas.2020.10.005 Lopresti, A. L., Smith, S. J., et al. (2019). An investigation into the stress-relieving and pharmacological actions of an ashwagandha extract. Medicine, 98(37), e17186. https://doi.org/10.1097/MD.0000000000017186 Pandit, S., Biswas, S., Jana, U., De, R. K., Mukhopadhyay, S. C., & Biswas, T. K. (2016). Clinical evaluation of purified shilajit on testosterone levels in healthy volunteers. Andrologia, 48(5), 570–575. https://doi.org/10.1111/and.12482 Saden-Krehula, M., Tajic, M., & Kolbah, D. (1971). Testosterone, epitestosterone and androstenedione in the pollen of Scotch pine Pinus sylvestris L. Experientia, 27(1), 108–109. https://doi.org/10.1007/BF02137731 Wankhede, S., Langade, D., Joshi, K., et al. (2015). Examining the effect of Withania somnifera supplementation on muscle strength and recovery: A randomized controlled trial. Journal of the International Society of Sports Nutrition, 12, 43. https://doi.org/10.1186/s12970-015-0104-9

Welcome to Episode 206 of the Homeopathy247 podcast! Today, host Mary Greensmith is joined by the wonderful homeopath Colleen Harris to discuss a surprising but incredibly common topic: urinary frequency and incontinence. If you have ever felt constantly tied to the bathroom despite having a clear medical checkup, this eye-opening episode is exactly what you need! The Mind-Body Connection Often, conventional medicine has very few answers for urinary frequency when there is no physical infection or pathology present. Colleen explains how our bladders can actually act as an emotional release valve. Deep-seated stress, feelings of injustice, sudden life transitions, or even a sense of betrayal can manifest physically as an uncontrollable or urgent need to go to the bathroom. Fascinating Real-Life Cases Colleen shares four unique cases that perfectly highlight how a tailored homeopathic remedy can resolve these stubborn issues: The 5-Year-Old Boy: After starting homeschool and facing a tough emotional transition, he began visiting the bathroom 20 to 30 times a day. A gentle dose of Calcarea Carbonica quickly brought his routine back to normal. The Successful Businessman: Waking up multiple times a night and struggling with daytime frequency, his symptoms were deeply tied to internal pressures. Lycopodium successfully cleared his symptoms and gave him his restful sleep back. The "Bursting Balloon" Incontinence: A woman dealing with sudden, uncontrollable incontinence triggered by an unfair work situation found profound relief and regained her control with the remedy Causticum. The Betrayal and UTIs: Another woman suffering from chronic UTIs (five in a single year) and involuntary urination following a deep personal betrayal found incredible healing and a cessation of accidents with the remedy Staphysagria. Why Individualized Remedies Matter As Colleen notes, there is no single generic "bladder remedy." Homeopathy looks at the timeline of your life—asking the vital detective question: "What happened right before these symptoms started?" By addressing the emotional root cause, your body can finally relax, rebalance, and naturally heal from the inside out. Important links mentioned in this episode: Visit Colleen's website: https://aurahomeopathy.life/ Know more about Colleen: https://homeopathy247.com/professional-homeopaths-team/colleen-harris/ Download Colleen's free ebook "Why Am I Peeing So Much?": https://free.homeopathy247.com/peeing-so-much You can also subscribe to our podcast channels available on your favourite podcast listening app below: Apple Podcast: https://podcasts.apple.com/us/podcast/homeopathy247-podcast/id1628767810 Spotify: https://open.spotify.com/show/39rjXAReQ33hGceW1E50dk Follow us on our social media accounts: Facebook: https://www.facebook.com/homeopathy247 Instagram: https://www.instagram.com/homeopathy247 You can also visit our website at https://homeopathy247.com/

Urinary incontinence affects about a third of adult women in Canada, yet many never receive a diagnosis or treatment. On this episode, Dr. Blair Bigham and Dr. Mojola Omole discuss the CMAJ review “Diagnosis and management of urinary incontinence in females,” which outlines how physicians can identify common forms of incontinence and begin management in primary care.The episode opens with Sharon Roman, who shares her experience living with bladder dysfunction related to multiple sclerosis. Her story highlights the embarrassment, health consequences and barriers to care that can come with urinary incontinence, as well as the frustration of being told to simply keep living with symptoms that profoundly affect quality of life.Dr. Louise-Helene Gagnon, an author of the review, a urogynecologist at Sunnybrook Hospital and assistant professor at the University of Toronto, explains the distinction between stress urinary incontinence and urge incontinence. She reviews common risk factors, including childbirth, menopause and pelvic floor injury, and walks through treatment options including pelvic floor physiotherapy, pessaries, mirabegron, vaginal estrogen and specialist referral.For physicians, the central message is simple: patients may not raise urinary incontinence on their own. Asking about it directly can open the door to practical treatments that reduce isolation, embarrassment and daily disruption.For more information from our sponsor, go to md.ca/lifeplanComments or questions? Text us.Join us as we explore medical solutions that address the urgent need to change healthcare. Reach out to us about this or any episode you hear. Or tell us about something you'd like to hear on the leading Canadian medical podcast.You can find Blair and Mojola on X @BlairBigham and @DrmojolaomoleX (in English): @CMAJ X (en français): @JAMC FacebookInstagram: @CMAJ.ca The CMAJ Podcast is produced by PodCraft Productions

Send us Fan MailIs five days of antibiotics enough to treat a urinary tract infection in a NICU infant? In this Journal Club episode, Ben and Daphna review a single-center study from Nationwide Children's Hospital examining adherence and safety of a five-day antibiotic treatment guideline for culture and urinalysis-proven UTIs in the NICU. Among 77 infants with 93 bacterial UTIs, the five-day course was associated with a 1% failure rate, defined as reinitiation of antibiotics within seven days for the same organism. The episode also explores the potential role of enteral antibiotic therapy and what shorter treatment courses could mean for babies still weeks away from discharge.----Urinary tract infection in the neonatal intensive care unit. Magers J, Burton A, Prusakov P, White NO, Miller RR, Moraille R, Theile AR, Sánchez PJ; Nationwide Children's Hospital Neonatal Antimicrobial Stewardship Program (NEO-ASP).J Perinatol. 2026 May;46(5):754-760. doi: 10.1038/s41372-026-02690-1. Epub 2026 Apr 29.PMID: 42056240 Free PMC article.Support the showAs always, feel free to send us questions, comments, or suggestions to our email: nicupodcast@gmail.com. You can also contact the show through Instagram or Twitter, @nicupodcast. Or contact Ben and Daphna directly via their Twitter profiles: @drnicu and @doctordaphnamd. The papers discussed in today's episode are listed and timestamped on the webpage linked below.Enjoy!
Are we prescribing medications for FIC that lack meaningful evidence? Dr. Serge Chalhoub, a board-certified small animal internal medicine specialist and Professor at the University of Calgary's Faculty of Veterinary Medicine, joins the Purr Podcast to discuss best practices in feline urinary disease management. His clinical and research interests focus on nephrology, urology, point-of-care ultrasound, and minimally invasive procedures. What should be first-line therapy for cats with lower urinary tract disease?Thanks for tuning in to the Purr Podcast with Dr. Susan and Dr. Jolle!If you enjoyed today's episode, don't forget to subscribe, rate, and leave us a review—it really helps other cat lovers and vet nerds find the show. Follow us on social media for behind-the-scenes stories, cat trivia, and the occasional bad pun. And remember: every day is better with cats, curiosity, and maybe just a little purring in the background. Until next time—stay curious, stay kind, and give your cats an extra chin scratch from us. The Purr Podcast – where feline medicine meets feline fun.

Urinary tract infections are one of the most common health issues women experience, yet there's still so much confusion about what they are, why they happen, and how they're different from yeast infections and other vaginal conditions. In this episode of Ask Dr. A, Dr. Aliabadi breaks down the anatomy behind UTIs, explains the difference between bladder infections and kidney infections, and shares the symptoms every woman should know.Dr. Aliabadi also dives into why some women seem to get recurrent UTIs while others never experience them, covering the roles of hydration, sex, genetics, hormones, menopause, and the vaginal microbiome. She explains how bacteria causes infection, why urine cultures are essential for an accurate diagnosis, and the common mistakes that can lead to repeated infections.Plus, you'll learn evidence-based prevention strategies, including the truth about cranberry supplements, D-mannose, vaginal estrogen, probiotics, and whether peeing after sex actually helps. If you've ever wondered why UTIs keep coming back, or how to lower your risk, this episode is packed with practical information every woman should know.Subscribe to SHE MD Podcast for expert tips on PMOS, endometriosis, fertility, hormonal balance, mental health, and more. Share with friends and visit SHE MD website and Ovii for research-backed resources, holistic health strategies, and expert guidance on women's health and well-being.SponsorsMidi: Ready to feel your best and write your second act script? Visit JoinMidi.com today to book your personalized, insurance-covered virtual visit. Peloton: Let yourself run, lift, sculpt, push and GO. Explore the new Peloton Cross Training Tread+ at onepeloton.comMyriad: List GetMyRisk.com to learn more about hereditary cancer testing and how you can use Myriad's virtual care option for fast, at-home testing - no office visit required. Talkiatry: Head to Talkiatry.com/shemd and complete the short assessment to get matched with an in-network psychiatrist in just a few minutes.Transcendental Meditation: Curious about Transcendental Meditation? Find a certified teacher near you and begin your journey today. Go to TM.org/SheMDWhat You'll LearnThe difference between UTIs, bladder infections, kidney infections, and yeast infectionsHow bacteria enters the urinary tract and causes infectionCommon UTI symptoms and warning signs you shouldn't ignoreWhy some women are more prone to recurring infectionsThe role of hydration, sex, and vaginal health in UTI preventionHow menopause and declining estrogen affect urinary tract healthWhen a urine culture is necessary and why it mattersThe truth about cranberry supplements, D-mannose, and other prevention strategiesWhy recurrent UTIs may require a deeper investigationKey Timestamps00:00 Welcome to She MD Podcast00:46 UTI, Yeast infection, Bladder infection, and Kidney infection07:12 E.coli and how you get them in the urethra13:09 How is the test called?19:45 What can a woman do for these infections?29:13 What kind of treatment will help with the infection?37:15 Vaginal Estrogen Treatment 45:18 How do you address the bacteria?50:20 How much is too much?51:40 Let's address some myths 53:33 Final WordsKey TakeawaysUTIs and yeast infections are completely different conditions that affect different parts of the body.Most UTIs begin as bladder infections caused by bacteria entering the urethra.Early diagnosis and treatment can help prevent serious kidney infections.Hydration, urinating after sex, and avoiding prolonged urine retention can reduce risk.Vaginal microbiome health plays a major role in preventing recurrent UTIs.Menopause-related estrogen loss can increase susceptibility to urinary tract infections.A urine culture is the best way to confirm whether symptoms are truly caused by a UTI.Cranberry extract and D-mannose may help prevent recurrent infections but are not treatments for active UTIs.Recurrent infections should prompt an evaluation of underlying causes rather than repeated rounds of antibiotics.See Privacy Policy at https://art19.com/privacy and California Privacy Notice at https://art19.com/privacy#do-not-sell-my-info.
Are we giving cats medications that don't actually help? Dr. Serge Chalhoub, a veterinary kidney and bladder specialist at the University of Calgary, joins the Purr Podcast to talk about the best ways to care for cats with urinary problems. He has a special interest in how cats' kidneys and bladders work, and in using bedside ultrasound -- think instant imaging right there in the exam room -- to get faster, clearer answers without putting cats through unnecessary procedures. Tune in to find out what really works -- and what might be nothing more than habit -- when your cat is having trouble in the litter box.

Welcome and thank you for listening! Urinary tract infections (UTIs) are incredibly common, but when they become a recurring nightmare—or flare up during pregnancy and postpartum—the stakes become much higher. Many women find themselves trapped in a cycle of repeated antibiotic use, relying on traditional remedies like cranberry juice that don't quite deliver. In this episode, we are busting the biggest myths around urinary tract health and diving deep into the science of prevention and treatment. Joining us is Jason Stewart, the driving force behind Probitec Health, to unpack the fascinating connection between the gut, the vaginal microbiome, and the bladder. We explore why pregnancy makes women more vulnerable to UTIs, the clinical risks of leaving them untreated, and the breakthrough science behind "Activated Cranberry" and advanced probiotic delivery. What We Discuss in This Episode: The Perinatal Vulnerability: Why UTIs are more common during pregnancy, why they become more serious, and the potential risks to both mother and baby. The Conception & Postpartum Window: Why addressing urinary and vaginal health before trying to conceive is crucial, and why these issues often flare up after giving birth. Busting the Cranberry Myth: The scientific reality of what cranberry actually does (hint: it doesn't kill bacteria!) and why most standard cranberry products fail. The Power of PACs: What Proanthocyanidins are, why dosage matters, and how they physically prevent bacteria from adhering to the urinary tract. The Microbiome Connection: Why combining 30 billion probiotic bacteria with cranberry is a game-changer for long-term urinary tract resilience. Delivery Technology Matters: What Phytosome® technology is and how it ensures active ingredients and probiotics actually survive to do their job. Resources Mentioned: Learn More about Probitec: ProBitec South Africa Part 1: Why Most Probiotics Fail: Gut Health & Your Second Brain If you found this episode helpful please leave us a review or give us a rating as that helps us get the show out to more people. And don't forget to subscribe! We'd love to stay in touch and keep you updated with all our latest content & resources to equip & empower you. So if you're a midwife or any type of birth and baby worker go to sensitivemidwifery.co.za/freegift If you're a mom, visit sisterlilian.co.za/freegift for more training and resources. That way we can keep you up to date when we release new episodes like this plus a few other bonuses. Remember you're making a big difference because you're shaping the future of humankind. Thanks for listening and I look forward to journeying with you.

Learn more about Parkinson's and find support: https://dpf.org In part three of this three-part series on Parkinson's and the senses, the panel covers vision changes like difficulty driving at night, light sensitivity, depth perception, and how DBS adjustments can affect focus. They also discuss vertigo, dizziness, and the urinary urgency that many people with Parkinson's experience but rarely talk about, including practical strategies like pre-boarding flights and planning bathroom access. Sign up for updates on webinars, events, and resources for the Parkinson's community: https://dpf.org/newsletter-signup Season 7 Episode 8 Davis Phinney Foundation, Copyright 2026

Welcome to episode two of The Women's Health Wellness Edit — a brand new Slightly Spiritual mini series bringing you real, honest conversations with some of the top experts in women's health, longevity, hormones, brain health, and modern wellness. Because frankly? Too many women are being told their exhaustion, brain fog, anxiety, inflammation, and burnout are “normal” — and we think it's time for a deeper conversation. In today's episode, we sit down with Ariana Thacker, founder and CEO of MoldCo, for one of our most requested conversations yet: mold illness, mold exposure, mycotoxins, CIRS, and the hidden ways our environments can impact our health. Ariana shares her personal journey with mold illness and how it ultimately led her to build MoldCo, a healthcare technology platform dedicated to helping patients identify and navigate mold toxicity. Together, we dive into why so many people, especially women and children, are experiencing chronic symptoms while being told their labs look “normal,” and why mold illness is still so misunderstood in modern medicine. We discuss the difference between mold allergy and mold illness, common mold symptoms, symptoms of mold allergies, what mycotoxins actually are, and how mold exposure can impact everything from brain fog and fatigue to anxiety and inflammation. Ariana also explains how everyone in the same household can present completely differently, how does black mold affect you, and whether mold is dangerous for long-term health. Ariana breaks down colonized mold, the genetic component that can make some people more susceptible to mold illness, and why mold is often referred to as “the great mimicker.” This episode also covers: * Symptoms of mold allergies and how they differ from mold toxicity * Mold illness in children * Proper home testing and why air sampling alone often misses the full picture * Signs mold may be hiding in your home * Urinary mycotoxin testing and key biomarkers for mold illness * The Shoemaker Protocol and Dr. Shoemaker's work * Mold remediation tips and what to look for in a remediator * How to reduce mold exposure while traveling or living in a moldy environment * The truth about “black mold” vs. other toxic molds * Is mold dangerous? Understanding risk factors and susceptibility Whether you're actively navigating mold illness, questioning unexplained symptoms, researching mold exposure, or simply wanting to better protect your family's health, this episode is packed with practical information, validation, and actionable advice. As always, this episode is not intended to replace medical advice, diagnosis, or treatment. Please consult your healthcare provider regarding your individual health concerns. Keep in touch with Ariana: Website: https://www.moldco.com/ Testing: https://www.moldco.com/products YouTube: https://www.youtube.com/@themoldcompany Free Questionnaire: https://access.moldco.com/signs MoldCo LinkedIn: https://www.linkedin.com/company/moldco/ Ariana's LinkedIn: https://www.linkedin.com/in/arianadthacker/ Instagram: https://www.instagram.com/themoldcompany/ Ariana's X: https://x.com/m0ldilocks MoldCo's X: https://x.com/themoldcompany A gift from Ariana: use code MOLDTEST10 for 10% off MoldCo's home dust test If this episode spoke to you, subscribe and leave a review on your favorite podcast platform or share it with a friend! podcasts.apple.com/us/podcast/slig…od/id1542525641 Follow us on Instagram: www.instagram.com/slightlyspiritualpod/ Follow Cindy on Instagram: www.instagram.com/revealingsoul/ Follow Ali on Instagram: www.instagram.com/alitmoresco/

A Parenting Resource for Children’s Behavior and Mental Health
Something feels off even when tests come back normal. Discover the hidden signs of PANS/PANDAS every parent misses as Dr. Nancy O'Hara unpacks sudden symptoms often mistaken for ADHD, anxiety, or autism. Dr. Roseann Capanna-Hodge, expert in Regulation First Parenting™, guides parents through emotional dysregulation and what to do next.Parents often know something is wrong—even when tests come back “normal.” In this powerful conversation with Dr. Nancy O'Hara, we explore the hidden signs of PANS/PANDAS every parent misses, and why so many children are misdiagnosed with ADHD, anxiety, or even autism.The truth? Sudden behavioral shifts, OCD, and physical symptoms may signal immune-driven brain inflammation—not “just behavior.” In this episode, you'll learn what PANS/PANDAS really is, how it affects the brain, and the overlooked signs parents and providers often miss. Why did my child suddenly change behavior overnight?When a child shifts abruptly—from calm to anxious, obsessive, or emotionally reactive—it can feel confusing and scary for parents.Dr. O'Hara explains that this sudden onset is a key marker of PANS/PANDAS, often triggered by infection or immune dysregulation.What parents should know:Sudden onset matters—changes can happen within days to weeksOCD, anxiety, or eating changes may appear quicklyIt's not bad parenting—it's a dysregulated immune responseTriggers may include strep, viruses, mold, or environmental stressorsReal-Life Example: A child who was once easygoing suddenly develops intense fears, refuses foods, or becomes highly anxious after an illness.As I always remind parents, behavior is communication—and sudden shifts deserve deeper investigation.Is OCD in kids always obvious—or can it be hidden?One of the most missed signs of PANS/PANDAS is hidden OCD, especially intrusive thoughts that don't look like typical compulsions.Dr. O'Hara emphasizes that many children suffer silently.Hidden OCD signs include:Intrusive, scary thoughts they can't explainWithdrawal, shutdown, or emotional overwhelmAvoidance of situations without clear reasonShame or embarrassment about thoughtsA child seems “anxious about everything,” but underneath is a looping fear they can't verbalize.This is where misdiagnosis often happens. It may look like generalized anxiety or even ADHD—but it's actually neurological inflammation affecting the brain's fear circuits.Let's be clear: your child is not choosing this. Their brain is overwhelmed.Why are medical tests normal if my child is struggling so much?This is one of the most frustrating experiences for parents—being told everything is “fine” when it clearly isn't.Dr. O'Hara explains that PANS/PANDAS is primarily a clinical diagnosis, not a lab-based one.Key insights:Bloodwork can look completely normalSome children cannot mount detectable immune responsesInflammation may still be present in the brainDiagnosis relies heavily on pattern recognition + historyReal-Life Example: A child with severe behavioral changes has “normal labs,” leading families to feel dismissed—despite clear real-world impairment.This is where validation matters. You're not imagining it.You don't have to figure this out alone.Become a Dysregulation Insider VIP and get your FREE Regulation Rescue Kit:How to Stay Calm When Your Child Pushes Your Buttons and Stop Oppositional Behaviors.Head to www.drroseann.com/newsletter and start your calm parenting journey today.What physical symptoms are easy to miss in PANS/PANDAS?Parents often focus on behavior and miss the body-based clues.Dr. O'Hara highlights that somatic symptoms are frequently overlooked—but incredibly important.Common missed signs:Urinary frequency or urgencyBedwetting after being drySleep disturbances or restless sleepHandwriting changes or regressionSensory overload or motor changesReal-Life Example: A child begins waking frequently at night and having bathroom accidents alongside new anxiety.These symptoms reflect nervous system dysregulation—not defiance or regression without cause.

Therapeutic Guidelines expert group member Lee Fong returns to the podcast to talk to Justin Coleman about the brand-new Kidney and Urinary guidelines. Focusing on GP management, the conversation covers some of the new content, including screening and medication regimens for chronic kidney disease, lower urinary tract symptoms, wetting in children and much more.

Host: Charles Turck, PharmD, BCPS, BCCCP Guest: Petros Grivas, MD, PhD Could emerging biomarkers redefine how we assess response and recurrence risk in muscle-invasive bladder cancer? To find out, Dr. Charles Turck speaks with Dr. Petros Grivas about the key findings from the phase 3 NIAGARA trial. Together, they explore how perioperative durvalumab impacts circulating tumor DNA (ctDNA) clearance and clinical outcomes, including event-free and overall survival. Their conversation also highlights the prognostic value of ctDNA and the potential for urinary tumor DNA to more closely correlate with pathologic complete response. Dr. Grivas is a Professor in the Division of Hematology and Oncology at the University of Washington School of Medicine, as well as the Clinical Research Division at the Fred Hutchinson Cancer Center, where he's also the Medical Director of the International Program and of local and regional outreach.

What if chronic illness was a path towards healing on levels greater than just physical? In this episode of Metabolic Matters, host Christina Mason sits down with Alekha Akkappedi and her longtime best friend, Emily Sullivan, for a powerful, multi-dimensional healing journey. At just 22 years old, pre-med student Alekha's life changed overnight. What began as a simple infection quickly spiraled into a complex web of chronic conditions: POTS, mast cell activation, PCOS, GERD, and connective tissue disease. Left bedridden, her science trained mind begins seeking answers. As she begins to experience healing in modalities outside of her allopathic education, she finds herself asking more questions and embarks on an unexpected career path. Alekha navigates years of uncertainty, traveling on paths that blend science, circadian biology, nutrition, and spiritual practices. Emily shares what it was like to watch her best friend's struggles and triumphs. Her perspective offers insight on the power of friendship and how watching another make healing choices vicariously heals those in close proximity. Alekha and Emily both experience healing as cyclical on many levels. Both agree that HOPE is one of the greatest healers. What unfolds for these two young sages is not just a story of physical recovery but transformation that is intangible, emotional and physical.After almost a decade of research and healing work, Alekha created the ALI Protocol, a comprehensive approach for those dealing with POTS, MCAS and long covid that integrates biology, psychology and energetic practices.

A big paper was published in the Lancet last month that has been circulating in the media with some PRETTY egregious headlines suggesting water isn't that important for kidney stones. Melanie dives into what this paper actually found and helps us understand WHY drinking water remains KEY to kidney stone prevention. Melanie's response on social media to doctors misrepresenting this research Desai AC, Maalouf NM, Harper JD, et al. Prevention of urinary stones with hydration: a randomised clinical trial of an adherence intervention. The Lancet. 2026;407(10534):1171-1181. Borghi L, Meschi T, Amato F, Briganti A, Novarini A, Giannini A. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study. J Urol. 1996;155(3):839-843. Submit a question for Melanie to answer on the podcast! Connect with The Kidney Dietitian! Work with Us! | Instagram | Facebook | Pinterest | Facebook Group | Newsletter www.thekidneydietitian.org FREE Webinar: The 3-Step Method to Prevent Kidney Stones All information in this podcast is meant for educational purposes only and should not be used in place of advice from a medical professional.

Ingenion Medical, run by our guest Ed Cappabianca, is going to change the standard catheter in the UK - The Foley catheter. Urinary catheter-associated infections kill 2,100 people a year and block 1.2 million hospital bed-days. And yet, the Foley catheter - the standard of care - has barely changed in 91 years. Ingenion Medical has built what replaces it.The cymactive™ 2.0R is a CE-marked, patient-controlled urethral catheter with a patented magnetic valve that is already in clinical use across the UK and 15 international markets. It is superior to either standard Foleys or intermittent catheters, and generates revenue today. Ingenion Medical are seeking investors. Here's the Investment case:• Revenue generative, regulatory approved. CE Mark achieved Q1 2024. ISO 13485 renewed October 2025. FDA pre-sub meeting completed.• Commercial traction. Distributor agreements in over 10 countries. NHS Supply Chain at contract award stage. 15 NHS hospitals active or in pipeline.• Profitable at 1,600 patients per month (80 urologists x 20 patients). Breakeven H2 2027. £49m revenue projected 2030.• Exit precedent. Comparable urology acquisitions: Urotronic > Laborie $600m;Neotract > Teleflex $1.1b; Augmenix > Boston Scientific $600m; .• World-class advisors. Advisory board includes: Professor Chris Chapple (former European Association of Urology Secretary General) and Professor Kurt Naber, global authority on urinary tract infections.If you would like the detailed Investor Pitch Deck, go to: ingenion.approvedinvestors.co.ukSummary of PodcastKey TakeawaysThe Problem: Current catheters cause frequent, costly infections (£2k–£3.5k per cycle for the NHS) and severely limit patient mobility and quality of life.The Solution: Ingenion's cymactive catheter is a 30-day, self-voiding device with no external bag, restoring patient dignity and designed to reduce infection risk.Market Validation: The NHS created a new framework channel specifically for SimActive, signaling strong support for its innovation and cost-saving potential.The Ask: Ingenion is raising £2M (for ~10% equity) to fund commercialisation, targeting a future trade sale to a major urology firm for a potential 10x investor return.The Problem with Current CathetersUrinary Retention: A common condition caused by issues like BPH (enlarged prostate), Parkinson's, MS, and spinal cord injuries.Foley Catheter (Indwelling):The 100-year-old standard, anchored by an internal balloon.Creates a "superhighway for bacteria," causing frequent, costly infections.Full cost of ownership for the NHS is ~£800/month per patient.Intermittent Catheters (Single-Use):Used 5–8 times daily, creating significant waste and inconvenience.Account for 90% (£157.5M) of the NHS's £175M annual catheter spend.Patient Impact:Fear of infection and public voiding → social isolation.Reduced fluid intake → dehydration, which can worsen conditions like dementia.The cymactive SolutionInnovation: A 30-day, self-voiding catheter with no external tubes or bags.Mechanism:An internal, patient-controlled magnetic valve.An external magnet opens the valve; removing it allows the valve to close naturally.Infection Defense:The urethra seals over the valve's end, mimicking the body's natural defense against bacteria.Anecdotal evidence suggests reduced infections and restored function.Product Pipeline:Current: cymactive for male urinary retention (CE marked).In Development: Versions for women and for male incontinence.Market Validation & CommercialisationNHS Adoption:The NHS created a new framework channel for cymactive, as it didn't fit existing categories.Ingenion was the sole applicant and signed a 2-year contract on March 12, 2026.Ordering codes are now live for hospitals.Go-to-Market Strategy:Goal: Build awareness among clinicians and patient groups.Method: Target early adopters and use their case studies, shared by the NHS innovation team, to drive broader adoption.Rationale: A randomised control trial was unfeasible because Foley catheter users were unwilling to risk being randomised to the control group.Investment OpportunityThe Ask: £2M for ~10% equity (pre-money valuation: £18M).Exit Strategy: Trade sale to a major urology firm (e.g., Coloplast, Becton Dickinson).Rationale: Leverage a large firm's infrastructure for rapid, global scaling.Target Return: A typical venture capital return of ~10x investment.Investor Profile: High Net Worth (HNW) or Sophisticated Investors.Due Diligence: Pitch deck available at ingenion.approvedinvestors.co.ukThe Next 100 Days Podcast Co-HostsGraham ArrowsmithGraham founded Finely Fettled in 2014 to provide data from The UK High Net Worth Database to marketers targeting affluent and high-net-worth customers. He's the founder of MicroYES, a Partner for MeclabsAI, creating lead generation AI Agents & Workflows and introducing the MeclabsAI Platform. Graham also provides an Answer Engine Optimisation solution to get your website in shape to be found by LLMs.Kevin ApplebyKevin specialises in finance transformation and implementing business change. He's the COO of GrowCFO, which provides both community and CPD-accredited training designed to grow the next generation of finance leaders. You can find Kevin on LinkedIn and at kevinappleby.com

Update Series (2026): Perioperative Management of Urinary Diversion: What Every Urologist Should Know Host: Mark L. Gonzalgo, MD, PhD, MBA Guest: Rohit Reddy, MD Now in its 45th installment, the AUA Update Series is renowned for delivering high-quality lessons to practicing urologists, fellows and residents. All content is developed by internationally recognized experts in urology, making the AUA Update Series the most professional and sought-after self-study program available. Improve your practice and patient care by staying abreast of the latest treatments and surgical techniques in urology. For more information or to subscribe to the AUA Update Series, please visit CME.auanet.org

Urinary incontinence affects more people than you'll ever know - but that doesn't mean it has to affect YOU. Learn why bladder leakage numbers are increasing, and what you can do if this condition is limiting your lifestyle. Core Restore City: Charleston Address: 675 Saint Andrews Boulevard Website: http://www.corerestorecenters.com Phone: +1 986 267 3737 Email: ann@corerestorecenters.com

Do all those supplements claiming to be “natural Adderall” actually do anything, or are they just giving you a much-needed dose of vitamin B? That's the question we're attempting to answer as we continue down the rabbit hole of supplements and ADHD. In an episode sponsored by the concept of multivitamins, Professor Kristin is covering the different types of vitamin B, what's happening at the molecular level, how vitamin B deficiencies impact the brain and body, and ways you can increase your intake without falling for supplement scams. Whether you're a liver and onions type of gal, you like to graze on fistfuls of leafy greens, or you prefer to get your nutrients the old-fashioned way via vitamin gummies, increasing your vitamin B can transform your energy levels for the better, no gimmicks required. Resources: Vitamin B-6 - ScienceDirect Attention-deficit hyperactivity disorder (ADHD) as a pyridoxine-dependent condition: Urinary diagnostic biomarkers - ScienceDirect Vitamins B9 and B12 in children with attention deficit hyperactivity disorder (ADHD): A systematic review: International Journal for Vitamin and Nutrition Research: Vol 94, No 5-6 Neurodevelopmental effects of maternal folic acid supplementation: a systematic review and meta-analysis: Critical Reviews in Food Science and Nutrition: Vol 63 , No 19 - Get Access The Impact of Maternal Folates on Brain Development and Function after Birth - PMC Prenatal Folic Acid Supplements and Offspring's Autism Spectrum Disorder: A Meta-analysis and Meta-regression - PubMed Maternal serum Vitamin B12 and offspring attention-deficit/hyperactivity disorder (ADHD) | European Child & Adolescent Psychiatry Serum Biomarker Analysis in Pediatric ADHD: Implications of Homocysteine, Vitamin B12, Vitamin D, Ferritin, and Iron Levels The Effects of Vitamin Therapy on ASD and ADHD: A Narrative Review | Bentham Science Publishers My Demoiselle crane (Karkare) (Chamkai) Konj Male calling his female

Guest Dr. John Gore and host Dr. Davide Soldato discuss JCO article, "12-Month Results from the CISTO Study Comparing Radical Cystectomy Versus Bladder-Sparing Therapy for Recurrent Non-Muscle Invasive Bladder Cancer," which compares radical cystectomy and bladder sparing therapy for patients with recurrent high-grade non-muscle invasive bladder cancer. Dr. Gore and Dr. Soldato focus on the study's patient-centered approach, eligibility criteria, and quality of life after treatment. TRANSCRIPT The disclosures for guests on this podcast can be found in the show notes. Dr. Davide Soldato: Hello and welcome to JCO After Hours, the podcast where we sit down with authors from some of the latest articles published in the Journal of Clinical Oncology. I am your host, Dr. Davide Soldato, medical oncologist at Ospedale San Martino in Genoa, Italy. Today, we are joined by JCO author Dr. John Gore, urologist at Fred Hutch Cancer Center and professor of urology at University of Washington School of Medicine. Today, we will be discussing the article titled, "Twelve-Month Results From the CISTO Study Comparing Radical Cystectomy Versus Bladder-Sparing Therapy for Recurrent High-Grade Non-Muscle-Invasive Bladder Cancer." Thank you for speaking with us, Dr. Gore. Dr. John Gore: Thank you so much for having me. Dr. Davide Soldato: So, I just want to jump right in. We know that patients who are diagnosed with recurrent high-grade non-muscle-invasive bladder cancer can be treated with two different approaches. So, one is radical cystectomy, and the other is bladder-sparing therapy. I just wanted to understand: what was the gap that you were trying to fill with this study? In particular, one point that is very important is that this study is very centered on the preference of the patients. Why did you choose this endpoint instead of going for more solid oncology-based endpoints? Dr. John Gore: Yeah, so CISTO was a study that was derived really organically from patient engagement. I think as a clinical gap in care, making a decision about when to pursue radical cystectomy for patients with non-muscle-invasive bladder cancer is a tough decision for us as clinicians. We did some engagement work partnered with the Bladder Cancer Advocacy Network and my partner Angela Smith, and found that it is also a huge gap for patients. You know, they are very anxious about recurrences, and the decision about when to take out the bladder is a very difficult one. We did an evidence synthesis and found that evidence guiding this decision is fairly limited. The reason we chose more of a patient-reported endpoint is several-fold. One is that we, as part of our engagement work, also worked with our patient survey network to identify outcomes that were important to patients. Some of those are the same outcomes that we care about as clinicians - recurrence-free survival and metastasis-free survival - but several outcomes came out that were more patient-centered. These were patient-reported outcomes such as the burden on my finances, the burden on my caregiver or loved one, and the ability to return to physical activities that are important to them. Part of what is unique about CISTO is that this was a contract with PCORI where we knew we would only have about 12-month outcomes for the majority of our patients. That is too early to really derive a lot of the clinical outcomes, but we are able to answer that patient-centered question of, "Am I going to be able to return to physical activities that are important to me?" And that was the genesis of that as the primary endpoint. Dr. Davide Soldato: So, who were the patients that were eligible to participate in the CISTO trial? What were the key eligibility criteria? This is very particular to this study because this was actually an observational study. Why did you think that such a pragmatic approach still can inform us on what is the best treatment approach for these patients? Dr. John Gore: The intent of CISTO was not necessarily to focus on the tightly defined BCG-unresponsive patient population. That is a clearly important patient population, but every day we are all faced in our real-world practice with patients with challenging, high-grade recurrences that don't fit neatly into that BCG-unresponsive box. The reason we chose a broader inclusion was to help doctors and patients answer these same questions they have when it doesn't fit nicely into this BCG-unresponsive category. You know, maybe their BCG exposure was two years ago, but now they are having a recurrence after intravesical chemotherapy. That is no less challenging a clinical conundrum, and we wanted to be able to enroll those patients. Other key inclusions were that all of the patients in CISTO had to have BCG at some point, and they had to have recent exposure to some adjuvant instillational or intravenous therapy like pembrolizumab. We also had some exclusions that were important. They couldn't be participating in a phase 2 clinical trial, and they couldn't have had a prior upper tract urothelial cancer. The other point about the observational trial design is I think a really important one. Part of our engagement work also asked patients about their willingness to randomize. There is a ton of literature in our history of trials that failed to accrue well when they were comparing a large-scale surgical intervention with a more conservative management strategy. What we found is only about 10% of patients would be willing to randomize when the clinical comparison is between radical cystectomy and bladder-sparing therapy. So it was very clear that an observational study design was the only way we were going to get evidence to inform clinical care when one of the key comparators was radical cystectomy. And so that is why we utilized the observational trial design. Dr. Davide Soldato: Starting to go deeper into the results, you mentioned before that the endpoint you chose for this trial was really centered on what patients thought was more important to them. In particular, the primary endpoint of the study was physical function as measured by the EORTC QLQ-C30 questionnaire. I just wanted to understand: first, did you have a solid hypothesis regarding how physical function could be impacted by either radical cystectomy or bladder-sparing treatments? And second, what were the key results of the study? Dr. John Gore: We figured that at 12 months after enrollment, given the burden and morbidity of a radical cystectomy, that patients in the radical cystectomy arm would have worse self-reported physical functioning than patients in the bladder-sparing therapy arm. We did hypothesize that some of our secondary outcomes might potentially be better after radical cystectomy, such as recurrence-free survival and potentially some other cancer-specific outcomes, because it is a more definitive management strategy. For our primary endpoint, however, we hypothesized that it would be worse. What we found, and the key finding of our study, is that at 12 months after enrollment, physical functioning was not different between patients undergoing radical cystectomy and patients undergoing bladder-sparing therapy, which is just important in terms of clinical counseling because it just means that you can tell your patients, "Gosh, if we could fast-forward your life six to nine months after this procedure, your physical functioning would be similar to as if you had been able to keep your bladder." Dr. Davide Soldato: And you mentioned that there were some key secondary endpoints of the study, which included both other dimensions of quality of life and also hard clinical outcomes. We mentioned metastasis-free survival, for example. Going a little bit into the key secondary quality of life outcomes, we know that radical cystectomy can impact physical functioning, but we also know that bowel, sexual symptoms, and also genitourinary symptoms might potentially be impacted by this type of treatment. We also know that, especially in a system like the US, financial toxicity can be a significant burden for patients. Considering the two different approaches, was radical cystectomy better also in other key secondary quality of life outcomes, and was financial toxicity different between the two arms? Dr. John Gore: Thank you for highlighting some of the really important secondary outcomes that I think are really important to trying to figure out what's best for your patients. Some of the main ones were some of the bladder cancer-specific quality of life outcomes you highlight. Urinary quality of life was worse at enrollment in patients in the radical cystectomy arm but was no different 12 months after. What is unique about how we measure that is we used an instrument called the Bladder Cancer Index because we're comparing a population of patients who have lost their bladder with a population of patients who have retained their bladder, and there are different considerations by gender. And so that instrument is agnostic to urinary diversion status and gender. We found that bowel function and sexual function were worse in the radical cystectomy arm. It appeared that bowel functioning was getting better to the point of near equivalence at 12 months in the radical cystectomy arm but was still inferior to bladder-sparing therapy, and that probably relates to the fact that we use the bowel as part of the urinary diversion, and that causes some transient disruption in bowel function. Financial toxicity is an outcome we weren't initially planning on having as part of the CISTO study, but based on that patient feedback, we made that one of our key secondary outcomes. That actually demonstrated superiority in the radical cystectomy arm. I think it's important that we remember that when we do bladder-sparing therapy, those patients are predisposed to a number of visits to our office, whether they're for instillational therapies or cystoscopy surveillance visits. Sometimes that involves the patient themselves, and sometimes that involves a caregiver. We live in an area with a very large geographic catchment, so sometimes that involves overnight hotel stays and airfare. It can be a particular burden, as you made mention, especially in our healthcare system. Dr. Davide Soldato: Going back to the quality of life dimensions and especially considering the different treatments, 50% of the patients received radical cystectomy with robotic surgery. Did you look a little bit into whether the type of surgery that they received might potentially impact on these dimensions of quality of life? Dr. John Gore: These are some questions that a lot of urologists have asked us in the surgical arm, related to surgical approach, so robotic versus open, and urinary diversion type. We sometimes reconstruct the urinary tract with an incontinent diversion called an ileal conduit where the urine drains tonically into a bag, and we sometimes do a continent diversion where someone typically will have a neobladder, where you reconstruct a sphere reservoir out of intestines and sew it to the urethra. About 20% of patients in the radical cystectomy arm in CISTO had a neobladder. We have not yet looked at specific surgical factors and some of those outcomes. That is one of the secondary analyses that we have planned, but we have not drilled into how different surgical approach factors can affect some of our outcomes. Fortunately, we have about 200 patients in the radical cystectomy arm, so it's enough patients that hopefully we can look at some of those factors in the future. Dr. Davide Soldato: Going back to the clinical endpoints, you mentioned that several of these were measured. There was metastasis-free survival, cancer-specific survival, and progression-free survival. We now have the data at 12 months. I am just wondering if you can comment on those when comparing the radical cystectomy with the bladder-sparing techniques. Dr. John Gore: I think importantly, bladder cancer-specific survival was very high in both arms, over 95% at one year. So both patient populations do very well in terms of cancer-specific and overall survival at one year. You know, when you take out the bladder, you're taking out a big source of recurrences. Not surprisingly, there was a marked reduction in recurrences in the radical cystectomy arm, so they had better recurrence-free survival. There actually was worse progression-free survival in the radical cystectomy arm, but there is a big asterisk to that. As you noted, it is an observational study, and one of the areas of imbalance in the study is that we had higher cancer severity in the radical cystectomy arm. So there was about a 20% rate of progression at the time of radical cystectomy to muscle-invasive and node-positive disease. Of those progressions, the overwhelming majority of them were progressions at the time of radical cystectomy, which I think speaks to a couple of important factors. Number one is the challenge in staging these patients. Our staging of non-muscle-invasive bladder cancer is very reliant on our resection. And so there is this risk of understaging our patients. Number two is just the challenge of decision making, that we fear losing our window of cure in this patient population, which is why we try to steer some patients toward radical cystectomy, and that progression figure kind of speaks to that. Dr. Davide Soldato: Also, one of the factors that was most common in the patients who received radical cystectomy was the presence of other high-risk features. For example, non-urothelial histology, which I think is something that in clinical practice we tend to fear a little bit in terms of recurrence, and so it might potentially bias a little bit towards proposing more strongly radical cystectomy to the patient. Another thing that I wanted to have a comment on, so this is not really in the paper, but I think it speaks a little bit to how the data will evolve over time. Do you imagine these clinical outcomes changing over time, and do you think that with higher maturity of these endpoints, this study might be even more informative when counseling patients regarding what they are obtaining with a radical cystectomy versus the other type of treatments? Dr. John Gore: You know, I think in this cancer universe, 12-month outcomes are great, but I think we all want to see two-year and five-year outcomes. We're very fortunate to supplement the work that we've done in the initial CISTO study, we're very fortunate that we've gotten supplementary funding from the National Cancer Institute to get long-term outcomes in this patient population. So we are continuing to follow all of our CISTO study patients to get two-year and five-year outcomes. What we expect to find is the accrual of new events in the bladder-sparing therapy arm. About 7% of patients in the bladder-sparing therapy arm underwent cystectomy in the first year, but that number will probably go up either as they have recurrences or progression events. We definitely expect the recurrence-free survival to continue to have superiority in the cystectomy arm, but we probably will see the progression events equilibrate as more progression events accrue in the bladder-sparing therapy arm. Maybe by five years, we hypothesize that we'll see clinical superiority in the radical cystectomy arm. By then, we might also see mortality events that separate bladder cancer-specific survival and overall survival between the two arms potentially. But we don't know. Hypothetically, cystectomy has its own downstream risks. It is a major reconstruction with some metabolic sequelae and renal functional sequelae, and so there may be some general medical events that accrue in the cystectomy arm that are also impactful. Dr. Davide Soldato: One other thing that I think should be complimented on this study is that you also looked at several other endpoints that might be important for patients. For example, anxiety symptoms and depression symptoms. Dr. John Gore: Yeah, I think one of the other key secondary outcomes we looked at were mental health outcomes. We utilized the PROMIS domains of anxiety and depression. Not unexpectedly, our radical cystectomy arm patients exhibited higher anxiety symptoms and higher depression symptoms at enrollment. What we found is at 12 months, they actually had significantly lower anxiety and depression than patients in the bladder-sparing therapy arm. We hypothesized in this paper that that actually relates probably mostly to cancer-specific anxiety. You know, when you experience this cavalcade of recurrences, it just breeds an anxiety about adverse cancer-specific outcomes, and by taking out the bladder, you kind of eliminate this prevalent source of anxiety. We followed up the study with a qualitative piece where we interviewed 50 patients and 20 caregivers. Based on those interviews, and that's just a sample of the patient population, it did seem to be cancer-specific anxiety that was driving a lot of those responses. Dr. Davide Soldato: I would like to end with a methodological consideration on your part because we said that this was an observational study. Frequently we tend to think that observational studies come with a lot of bias, and so we tend to downgrade a little bit the results. But I think that a lot of the merit that goes in the CISTO study that was published in the JCO, and I think it also speaks to the fact that this is very high-quality data, comes with the fact that the methodology behind this study was really robust in terms of informing us. Even with this observational study that, as you said, was the only one that we could perform considering the patient population. So just a comment on your part also to speak to the solidity of the data that was published. Dr. John Gore: Importantly, you know, if you look at ClinicalTrials.gov or other sources, CISTO is the only trial that has radical cystectomy as a major comparator. In many ways, this study is our only source of evidence for radical cystectomy. So we'd rather have flawed observational evidence than no evidence at all. We all experience flaws of our RCTs as well. They tend to be these narrowly defined patient populations that may not match the patient in front of you. So I think there are unrecognized flaws on the other side as well. The way that we try to counterbalance that, and none of these techniques are perfect, but we used a strategy called 'targeted maximum likelihood estimation'. Like many methods, such as propensity scores or instrumental variable analysis, what we're trying to do theoretically is coax randomization from non-randomized data. And TMLE, which is the technique we use, tends to be pretty robust to that. So it's the best available way that we can try to counterbalance the bias based on age and clinical severity between the two patient arms. I also think what's important about this is that even when there are biases, I think we are able to infer those out and still extract meaningful details from the data. So even with the biased data, I think we all glean some really important clinical learnings from it. Dr. Davide Soldato: Absolutely, but I would also say that in terms of observational data, the work that you have done is really something that makes us quite confident about what you found in the CISTO study. So with this, I would like to thank you again for joining us today. Dr. John Gore: Thank you so much, and thank you for highlighting the CISTO study. We are very excited about the data. Dr. Davide Soldato: So Dr. Gore, we appreciate you sharing more on your JCO article titled, "Twelve-Month Results From the CISTO Study Comparing Radical Cystectomy Versus Bladder-Sparing Therapy for Recurrent High-Grade Non-Muscle-Invasive Bladder Cancer." If you enjoy our show, please leave us a rating and review and be sure to come back for another episode. You can find all ASCO shows at asco.org/podcasts. The purpose of this podcast is to educate and to inform. This is not a substitute for professional medical care and is not intended for use in the diagnosis or treatment of individual conditions. Guests on this podcast express their own opinions, experience, and conclusions. Guest statements on the podcast do not express the opinions of ASCO. The mention of any product, service, organization, activity, or therapy should not be construed as an ASCO endorsement. Guest Disclosure Dr. Gore:Consulting or Advisory Role: Astellas Pharma

Rich — a leukemia survivor, nurse practitioner, and longtime oncology clinician — to talk about what it's really like to survive cancer, rebuild your life after treatment, and live with long-term side effects.Rich was diagnosed with leukemia at age 28, underwent an allogeneic stem cell transplant at Dana-Farber / Brigham and Women's, and is now a 29-year survivor. His experience as both a patient and provider offers a rare, honest look at cancer survivorship, prostate cancer side effects, sexual health, mental health, and post-traumatic growth.In this conversation, we cover:What it's like to be told you have leukemia in your 20sStem cell transplant and long-term survivalTurning cancer into purpose and becoming an oncology NPCommon prostate cancer side effects (urination, bowel changes, erectile dysfunction)How doctors actually manage these symptomsSexual health after cancer treatmentMental health, grief, and post-traumatic growthHow to rebuild your life after active treatmentThis episode is for patients, survivors, caregivers, and anyone navigating life after a cancer diagnosis.
Update Series (2026) Lesson 5: Long-term Urinary Catheters: Their Role & Management of Complications Now in its 45th installment, the AUA Update Series is renowned for delivering high-quality lessons to practicing urologists, fellows and residents. All content is developed by internationally recognized experts in urology, making the AUA Update Series the most professional and sought-after self-study program available. Improve your practice and patient care by staying abreast of the latest treatments and surgical techniques in urology. For more information or to subscribe to the AUA Update Series, please visit https://cme.auanet.org/URL/US2026

The EV-303 trial that led to the FDA approval of perioperative enfortumab vedotin + pembrolizumab in cisplatin-ineligible bladder cancer patients in now published in NEJM. We discuss the results and ponder potential future changes to treating bladder cancer in the future. Urinary diversion surgeries: https://jamanetwork.com/journals/jamaoncology/fullarticle/2842595

Join the Buff Muff Community and stop letting your bladder run your life! https://get.buffmuff.com/methodSupport your pelvic and whole body health with Rejeuve https://rejeuve.com/Rejuve is a line of pelvic health and whole body health supporting supplements that are helping women have a daily poogasm, eliminate leaks and prolapse symptoms, and keep their vulvovaginal tissues supple and resilient. Get your Rejeuve Supplements https://rejeuve.com/ and use code Podcast to save 10% off your first order.Thank you so much for listening! I use fitness and movement to help women prevent and overcome pelvic floor challenges like incontinence and organ prolapse. There is help for women in all life stages! Every Woman Needs A Vagina Coach! Please make sure to LEAVE A REVIEW and SUBSCRIBE to the show for the best fitness and wellness advice south of your belly button. *******************I recommend checking out my comprehensive pelvic health education and fitness programs on my Buff Muff AppYou can also join my next 28 Day Buff Muff Challenge https://www.vaginacoach.com/buffmuffIf you are feeling social you can connect with me… On Facebook https://www.facebook.com/VagCoachOn Instagram https://www.instagram.com/vaginacoach/On Twitter https://twitter.com/VaginaCoachOn The Web www.vaginacoach.comGet your Feel Amazing Vaginal Moisturizer Here

Urinary tract infections are one of the most common reasons people with dementia end up in the emergency room. In this video, I talk with Dr. Krieger, an emergency room physician, about why UTIs often look different in dementia and why sudden changes should not automatically be blamed on dementia progression. Dr. Krieger is also the creator of Uraguard, a product designed to help reduce bacterial exposure around the urethra for women with incontinence. We talk about where tools like this may fit into UTI prevention, along with other practical strategies caregivers can use. Learn more about Uraguard here: https://tinyurl.com/uraguard-careblazers-yt

The first women's public toilets in London opened on Bedford St on 11th February, 1852 - attempting to capitalize on the success of George Jennings' ‘monkey closets', used by over 800,000 visitors to the 1851 Great Exhibition. Unfortunately, even though the facility had been fought for by campaigning women's sanitary organizations, middle and upper class Victorian ladies were not yet prepared to pee in public - and the toilets closed a year later. In this episode, Arion, Rebecca and Olly explain where the phrase ‘spending a penny' (probably) comes from; reveal why ‘the urinary leash' came to describe the predicament of women's lives; and investigate why the number of 21st century public toilets continues to fall… Further Reading: • ‘Pamphlets of the Ladies Sanitary Association' (Wellcome Collection): https://wellcomecollection.org/works?query=%22Ladies+Sanitary+Association.%22 • ‘London's long-term lav affair: A history of public toilets in the capital' (BBC News, 2022): https://www.bbc.co.uk/news/uk-england-london-59785477 • ‘Victorian realities - how did they use the toilet??!' (Prior Attire, 2016): https://www.youtube.com/watch?v=NUHeSTDv_24 Love the show? Support us! Join

Dr. Surell Levine graduated from Brown University with a Bachelor of Arts in 2001 and earned her Doctor of Veterinary Medicine from the University of Pennsylvania School of Veterinary Medicine in 2009. Following graduation, she completed a fellowship in Emergency and Critical Care and worked in the Emergency Room and Intensive Care Unit at Massachusetts Veterinary Referral Hospital. She is a certified veterinary medical acupuncturist and an active volunteer with the MSPCA animal shelter. She is also the inventor of the widely used Calm & Cozy Cat Wrap, a patented swaddle designed to make veterinary visits less stressful for cats. Topics covered in this episode: Preview of Dr. Surell's conference lecture on urinary sample collection and case management in house call practice Different styles of house call medicine, showing there's no single "right" way to practice Common urinary issues seen in home visits, including UTIs, cystitis Practical urine collection strategies in the home Using ultrasound as a quick in-home screening tool for urinary red flags Real-world urinalysis interpretation Balancing gold-standard preventive care with client budgets and real-life practice challenges Links & Resources: Calm & Cozy Cat Wrap: https://calmcozycat.com/ Hopkinton Home Vet https://www.hopkintonhomevet.com/ The House Call Vet Academy Resources: Download Dr. Eve's FREE House Call & Mobile Vet Biz Plan Find out about the House Call Vet Academy online CE course Learn more about the Concierge Vet Mastermind Get your FREE Concierge Vet Starter Kit mini course Learn more about Dr. Eve Harrison Learn more about 1-to-1 coaching for current & prospective house call & mobile vets Learn more about the House Call & Mobile Vet Virtual Conference → Register TODAY for the House Call & Mobile Vet Virtual Conference, February 7th-8th, 2026!!!!!! Music: In loving memory of Dr. Steve Weinberg. Intro and outro guitar music was written, performed, and recorded by house call veterinarian Dr. Steve Weinberg. This podcast is also available in video on our House Call Vet Cafe YouTube channel P.S. Here's a special gift from me as a huge thank you for being a part of our wonderful House Call Vet Cafe podcast community! ☕️ GET 20% OFF your Four Sigmatic Mushroom Coffee when you order through this link! 4Sig truly is my favorite!!! Enjoy it in good health, my friends!
Forever Young Radio Show with America's Natural Doctor Podcast
Millions of Americans are frustrated with their urinary problems. More specifically, the need to urinate multiple times a day and night and leaking urine is frustrating to many people over the age of 45. Fortunately, there have been successful advances in the herbal treatment of common urinary problems. We are excited to share these breakthroughs on the show today. Tracey Seipel, ND, is CEO and founder of Australian-based Seipel Group. Dr. Seipel is a renowned naturopathic doctor, medical herbalist, and clinical nutritionist. Dr. Seipel is also a diabetes educator, researcher, and an award-winning natural products formulator with 35 years of experience in clinical practice.She pioneered the natural urological health category receiving a Nutrition Business Journal award in 2006 for innovation. During the 1990s, Seipel was a leader in establishing standards of education for Australian naturopathic colleges and as an advisor to government boards, including developing nutritional training for Australia Medical Schools. During her research as a product formulator for nutraceutical companies, she uncovered the significant prevalence and underreporting of urinary incontinence in women and then overactive bladder and incontinence in both men and women. Together, this led to her pioneering this natural health category. Understanding the significant health impacts and seeing no other companies willing to take on the challenge of improving bladder control, Seipel developed the initial formulation.Learn more about UROXUROX StudyLearn more about Emerald Labs Bladder Health which contains the branded ingredient UROX. Listeners can save 20% OFF at Emeraldlabs.com when using the code: Forever

本集特別邀請到 台中榮民總醫院 婦產科暨婦女泌尿專科醫師——謝筱芸醫師,一起深入探討糖尿病對女性骨盆健康的影響。許多糖尿病女性常出現頻尿、急尿、漏尿或反覆泌尿道感染,這些症狀究竟是來自血糖控制不良、神經病變,還是骨盆底功能障礙?本集從臨床實務出發,說明常見泌尿症狀的鑑別診斷重點,並分享婦女泌尿科醫師如何與骨盆復健、內科新陳代謝科及家醫科跨團隊合作,協助病患在藥物治療與生活調整之間取得平衡。節目也特別談到:雖然部分排糖藥物可能增加泌尿道感染風險,但血糖控制不良對泌尿與骨盆健康的影響更為關鍵。如何在診斷、治療與提升病患遵醫囑性之間取得臨床平衡,是照顧糖尿病女性不可忽視的一環。

Chegou o episódio escolhido por vocês! Marcela Belleza e Joanne Alves convidam Carol Millon para conversar sobe 6 clinicagens de inibidores de SGLT2, as gliflozinas:Indicações além do DMRisco de CAD euglicêmicaQuando não usar?Cuidados com doença aguda (sick day) e hipovolemiaCuidados pré-operatórioRisco de fratura e amputaçãoReferências:1. Bailey CJ, et al. Dapagliflozin add-on to metformin in type 2 diabetes inadequately controlled with metformin: a randomized, double-blind, placebo-controlled 102-week trial. BMC Med. 2013;11:43. Published 2013 Feb 20. doi:10.1186/1741-7015-11-432. Bersoff-Matcha SJ, et al. Fournier Gangrene Associated With Sodium-Glucose Cotransporter-2 Inhibitors: A Review of Spontaneous Postmarketing Cases. Ann Intern Med. 2019;170(11):764-769. doi:10.7326/M19-00853. Chang HY, et al. Association Between Sodium-Glucose Cotransporter 2 Inhibitors and Lower Extremity Amputation Among Patients With Type 2 Diabetes. JAMA Intern Med. 2018;178(9):1190-1198. doi:10.1001/jamainternmed.2018.3034 4. Clar C, et al. Systematic review of SGLT2 receptor inhibitors in dual or triple therapy in type 2 diabetes. BMJ Open. 2012 Oct 18;2(5):e001007. doi: 10.1136/bmjopen-2012-001007. PMID: 23087012; PMCID: PMC3488745.5. Das SR, et al. 2020 Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients With Type 2 Diabetes: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020 Sep 1;76(9):1117-1145. doi: 10.1016/j.jacc.2020.05.037. Epub 2020 Aug 5. PMID: 32771263; PMCID: PMC7545583. 6. Fralick M, et al. Risk of amputation with canagliflozin across categories of age and cardiovascular risk in three US nationwide databases: cohort study. BMJ. 2020;370:m2812. Published 2020 Aug 25. doi:10.1136/bmj.m28127. Li D, et al. Urinary tract and genital infections in patients with type 2 diabetes treated with sodium-glucose co-transporter 2 inhibitors: A meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2017;19(3):348-355. doi:10.1111/dom.128258. Neal B, et al. Rationale, design, and baseline characteristics of the Canagliflozin Cardiovascular Assessment Study (CANVAS)--a randomized placebo-controlled trial. Am Heart J. 2013;166(2):217-223.e11. doi:10.1016/j.ahj.2013.05.0079. Nyirjesy P, et al. Evaluation of vulvovaginal symptoms and Candida colonization in women with type 2 diabetes mellitus treated with canagliflozin, a sodium glucose co-transporter 2 inhibitor. Curr Med Res Opin. 2012;28(7):1173-1178. doi:10.1185/03007995.2012.69705310. Perkovic V, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019;380(24):2295-2306. doi:10.1056/NEJMoa181174411. Rosenwasser RF, et al. SGLT-2 inhibitors and their potential in the treatment of diabetes. Diabetes Metab Syndr Obes. 2013 Nov 27;6:453-67. doi: 10.2147/DMSO.S34416. PMID: 24348059; PMCID: PMC3848644.12. Sridharan K, Sivaramakrishnan G. Risk of limb amputation and bone fractures with sodium glucose cotransporter-2 inhibitors: a network meta-analysis and meta-regression. Expert Opin Drug Saf. 2025;24(7):797-804. doi:10.1080/14740338.2024.237775513. Ueda P, et al. Sodium glucose cotransporter 2 inhibitors and risk of serious adverse events: nationwide register based cohort study. BMJ. 2018;363:k4365. Published 2018 Nov 14. doi:10.1136/bmj.k436514. Watts NB, et al. Effects of Canagliflozin on Fracture Risk in Patients With Type 2 Diabetes Mellitus. J Clin Endocrinol Metab. 2016 Jan;101(1):157-66. doi: 10.1210/jc.2015-3167. Epub 2015 Nov 18. PMID: 26580237; PMCID: PMC4701850.15. Zhuo M, et al. Association of Sodium-Glucose Cotransporter-2 Inhibitors With Fracture Risk in Older Adults With Type 2 Diabetes. JAMA Netw Open. 2021;4(10):e2130762. Published 2021 Oct 1. doi:10.1001/jamanetworkopen.2021.3076216. Emerson Cestari Marino, Leandra Anália Freitas Negretto, Rogério Silicani Ribeiro, Denise Momesso, Alina Coutinho Rodrigues Feitosa, Marcos Tadashi Kakitani Toyoshima, Joaquim Custódio da Silva Junior, Sérgio Vencio, Marcio Weissheimer Lauria, João Roberto de Sá, Domingos A. Malerbi, Fernando Valente, Silmara A. O. Leite, Danillo Ewerton Oliveira Amaral, Gabriel Magalhães Nunes Guimarães, Plínio da Cunha Leal, Maristela Bueno Lopes, Luiz Carlos Bastos Salles, Liana Maria Torres de Araújo Azi, Amanda Gomes Fonseca, Lorena Ibiapina M. Carvalho, Francília Faloni Coelho, Bruno Halpern, Cynthia M. Valerio, Fabio R. Trujilho, Antonio Carlos Aguiar Brandão, Ruy Lyra e Marcello Bertoluci. Rastreamento e Controle da Hiperglicemia no Perioperatório – Posicionamento Conjunto da Sociedade Brasileira de Diabetes (SBD), Sociedade Brasileira de Anestesiologia (SBA) e Associação Brasileira para o Estudo da Obesidade e Síndrome Metabólica (ABESO). Diretriz Oficial da Sociedade Brasileira de Diabetes (2025). DOI: 10.29327/5660187.2025-10 , ISBN: 978-65-5941-367-6.17. Singh LG, Ntelis S, Siddiqui T, Seliger SL, Sorkin JD, Spanakis EK. Association of Continued Use of SGLT2 Inhibitors From the Ambulatory to Inpatient Setting With Hospital Outcomes in Patients With Diabetes: A Nationwide Cohort Study. Diabetes Care. 2024;47(6):933-940. doi:10.2337/dc23-112918. Mehta PB, Robinson A, Burkhardt D, Rushakoff RJ. Inpatient Perioperative Euglycemic Diabetic Ketoacidosis Due to Sodium-Glucose Cotransporter-2 Inhibitors - Lessons From a Case Series and Strategies to Decrease Incidence. Endocr Pract. 2022;28(9):884-888. doi:10.1016/j.eprac.2022.06.00619. Umapathysivam MM, Morgan B, Inglis JM, et al. SGLT2 Inhibitor-Associated Ketoacidosis vs Type 1 Diabetes-Associated Ketoacidosis. JAMA Netw Open. 2024;7(3):e242744. Published 2024 Mar 4. doi:10.1001/jamanetworkopen.2024.274420. Fleming N, Hamblin PS, Story D, Ekinci EI. Evolving Evidence of Diabetic Ketoacidosis in Patients Taking Sodium-Glucose Cotransporter 2 Inhibitors. J Clin Endocrinol Metab. 2020;105(8):dgaa200. doi:10.1210/clinem/dgaa20021. Neuen BL, Young T, Heerspink HJL, et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2019;7(11):845-854. doi:10.1016/S2213-8587(19)30256-622. Braunwald E. Gliflozins in the Management of Cardiovascular Disease. N Engl J Med. 2022;386(21):2024-2034. doi:10.1056/NEJMra211501123. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015;373(22):2117-2128. doi:10.1056/NEJMoa150472024. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med. 2017;377(7):644-657. doi:10.1056/NEJMoa161192525. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2019;380(4):347-357. doi:10.1056/NEJMoa181238926. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med. 2019;381(21):1995-2008. doi:10.1056/NEJMoa191130327. Packer M, Anker SD, Butler J, et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N Engl J Med. 2020;383(15):1413-1424. doi:10.1056/NEJMoa202219028. Anker SD, Butler J, Filippatos G, et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N Engl J Med. 2021;385(16):1451-1461. doi:10.1056/NEJMoa210703829. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020;383(15):1436-1446. doi:10.1056/NEJMoa202481630. The EMPA-KIDNEY Collaborative Group, Herrington WG, Staplin N, et al. Empagliflozin in...

Fear isn't just a thought.For many women, fear is a body pattern — and it often lives in the kidneys, adrenals, pelvic floor, and urinary system.In this episode of The Sovereign Sisterhood Movement Podcast (Body Systems + Generational Healing Series), I'm breaking down — in simple language — how your urinary system is actually one of your body's main survival + safety systems.What you'll learn in this episode:-Why anxiety and chronic stress can show up as a kidney/adrenal pattern (not a “weak mindset”)-How generational trauma trains the body to stay on alert (and why it feels like you can't relax even when life is “fine”)-The urinary system basics: kidneys, bladder, urethra, pelvic floor — and what they're doing all day to keep you alive-How cortisol + adrenaline overload the system (and why dehydration can make anxiety louder)-The Root Chakra connection (safety, support, trust, survival) through trauma-informed Kundalini Yoga Therapy-The faith over fear reframe through A Course in Miracles spiritual psychotherapy: how faith can become chemical, not just spiritual-A simple, supportive kidney-nourishing practice + recipe you can start integrating right awayNow here's your Permission (because you might be in the “I didn't even know this was a thing” stage)-If you've been blaming yourself for being “too anxious,” “too tense,” or “unable to rest”…you're not broken.Your body may have been trained, for generations, to live like danger is always around the corner.And the good news is: the body can be re-educated. Safety can be rebuilt. Faith can be embodied. Your nervous system and brain can learn a new normal.Want support doing this work with structure + sisterhood?I'm Veronica Barragán, trauma-informed Kundalini Yoga Therapist and founder of The Sovereign Sisterhood Sanctuary, an online sanctuary for first-time cycle breakers healing rewiring their nervous system + brain from generationla trauma body + mind + spirit.If this episode hit home, your next step is simple:✨ Join us inside the Sanctuary (link below) and start rebuilding safety from the inside out.

Title: Comparative assessment of routine H&E and Mason's Trichrome Stain to Differentiate Normal from Infected Urinary Bladders in the Göttingen Minipig Authors: Stephanie D. Rivera, MS, HT(ASCP); Anthony Romanello, BS; Ronnie Chamanza, BVSc, MSc, FRC Path, MRCVS, FIATP, Preclinical Sciences & Translational Safety, Johnson & Johnson Innovative Medicine, Spring House, Pa Abstract: The objective of this experiment was to evaluate the difference between normal and infected Göttingen minipig urinary bladder and determine the difficulty of microscopically evaluating infectious urinary bladder. The focus was on the histology of the tissue using routine Hematoxylin and Eosin(H&E) staining and the Masson Trichrome (MT) special stain to demonstrate the morphology of normal and infectious urinary bladder. To improve on the translation between preclinical and clinical studies, the Göttingen minipig model is appropriate to use for research for diseased human bladder treatment because the minipig anatomy and organ system are similar to humans. The procedure was designed to evaluate normal uninfected urinary bladder and bacteria infected (E. coli) urinary bladder by evaluating morphology/cellular changes associated with the resultant inflammatory response in the urinary bladder of the Ellegaard Gottingen Minipig. The H&E-stained urinary bladder tissue section and a Masson Trichrome stained urinary bladder section were used to evaluate control ‘normal' tissue vs infected tissue cellular differences. Optimal microscopic evaluation requires that the urinary bladders are properly fixed and processed. By using proper fixation and diligent histologic practices, all components of the urinary bladder are captured for proper histologic evaluation.
Send us a textIn this episode, Dr. Andrew Beverstock discusses his research on urinary sodium and its relationship with growth in preterm neonates. He shares insights into the importance of sodium for neonatal growth, the methodology of his study, and the unexpected results that challenge existing literature. The conversation also touches on his diverse medical training, mentorship experiences, and his involvement in medical education and point-of-care ultrasound (POCUS). Dr. Beverstock emphasizes the significance of careful population selection in research and outlines his future research directions. Support the showAs always, feel free to send us questions, comments, or suggestions to our email: nicupodcast@gmail.com. You can also contact the show through Instagram or Twitter, @nicupodcast. Or contact Ben and Daphna directly via their Twitter profiles: @drnicu and @doctordaphnamd. The papers discussed in today's episode are listed and timestamped on the webpage linked below. Enjoy!
On this month's EM Quick Hits podcast: Deborah Schonfeld on the differential diagnosis and work up of pediatric urinary retention & acute transverse myelitis, Jesse McLaren on his Tryptic Approach to Occlusion MI Diagnosis, Matthew McArthur on recognition and management of post-dural puncture headache, Joseph Yasmeh on Med Mal Cases: Clenched fist injury, Brit Long on IV thrombolysis for minor strokes and Victoria Myers & Lauren Westafer on mentorship and what it means to be a physician leader... Please consider a donation to EM Cases to support high quality Free Open Access Medical Education here: https://emergencymedicinecases.com/donation/
Why do so many indoor cats develop urinary disease? Meet Dr. Allison Kendall, Associate Professor of Internal Medicine at NC State and feline nephrology & urology specialist. In this episode of Purr Podcast, we talk pee, pain, and common causes for urinary probems in cats.

Pre-Order The Forever Strong PLAYBOOK and receive exclusive bonuses: https://drgabriellelyon.com/playbook/Want ad-free episodes, exclusives and access to community Q&As? Subscribe to Forever Strong Insider: https://foreverstrong.supercast.comIn this compilation episode, Dr. Gabrielle Lyon is joined by the top experts in Testosterone and men's health treatments. You'll learn:Why aging alone doesn't drop T levels and why acquisition of conditions like obesity is the real culprit.Why the standard "low T" cutoff is misleading and why you must check your Free Testosterone.How erectile dysfunction is a sensitive marker of overall health and heart risk.The efficacy of Cialis/Viagra for both erections and cardiac protection, and the risks of unchecked influencer advice on steroids.The direct link between muscle mass, exercise, and sexual function—and why the penis is the "first to go" when overall health declines.Chapter Markers:0:00 - Testosterone is a Brain Hormone0:40 - Debunking the Myth: Male Menopause (Andropause) Doesn't Exist1:33 - The Dangers of Unchecked Influencer Advice on Testosterone3:07 - Defining Testosterone Deficiency: Symptoms vs. Signs5:10 - The Arbitrary Number: Why Guidelines Disagree on Low T8:29 - Free Testosterone: The Most Reliable Indicator of Male Health15:28 - TRT vs. Steroids: Defining the Line and Risks18:59 - The Real Risks of TRT: Infertility and Hematocrit22:36 - The Shocking Backstory: Challenging the Prostate Cancer Myth26:40 - Erectile Dysfunction (ED) and Lifestyle Modification29:21 - Shockwave Therapy for ED: The Science and the Cash Business33:53 - Penile Tissue Atrophy and Venous Leak37:25 - The Role of Muscle Mass, Sarcopenia, and Sexual Function39:41 - The Single Best Marker for Male Health: Erectile Function42:02 - The Science of Cialis and Viagra (PDE5 Inhibitors)45:49 - The Viagra Story: From Heart Drug to ED Cure50:50 - Tadalafil (Cialis) as a Triple-Threat Drug (Cardiac, Urinary, Sexual)53:57 - The Role of Testosterone in Female Sexual Function55:20 - Hypogonadism: Diagnosis, Treatment, and Fertility RiskAbout the guests: Dr. Abraham Morgentaler is an Associate Clinical Professor of Urology at Harvard Medical School and founder of Men's Health Boston. He is an internationally recognized expert in men's health, particularly known for his pioneering work in testosterone therapy. Dr. Morgentaler is credited with reversing the long-held belief that testosterone therapy causes prostate cancer and is the author of several books on men's health. YouTubeLinkedInT4L EducationX/Twitter Dr. Tobias Kohler is the co-founder of the Erectile Restoration Outcomes Study (EROS) penile implant registry. In addition to his clinical and research activities, Dr. Kohler is active in education, providing mentorship to residents and fellows.Mayo Clinic ResearchGateLinkedIn

Send us a textOver 200 million people worldwide suffer from incontinence but few seek treatment or education. Urinary incontinence is not age related and is manageable and treatable without surgery. Want more education and resources: nafc.org Support the showSeniorSupportStrategies.com when you need guidance navigating senior care or how to create your own Aging in Place strategy.

Urinary (and yes, bowel) leakage isn't “just part of getting older”—it's a signal from your core and pelvic floor. In this straight-talk episode, physical therapist Christina Walsh, co-founder of Tighten Your Tinkler, joins me to dismantle the shame around pelvic health and lay out a functional path forward that goes far beyond “just do more Kegels.” We cover what's really driving leaks, pressure, prolapse, urgency, and painful sex in midlife; how breath, posture, fascia, and daily toileting habits influence symptoms; when conservative care is enough—and when devices, pessaries, or surgery may be appropriate. Christina also shares practical first steps you can start today (hello, decompression and diaphragmatic breathing), plus how to talk with your partner without pushing through pain.What you'll learnWhy leaking is common—but not normal—and what it's trying to tell youThe limits of isolated Kegels and what a functional approach looks likeHow breathing, posture, sitting, and constipation ramp up pelvic pressureStaging prolapse (1–4), what's realistic to “functionally heal,” and red-flagsPainful sex in midlife: estrogen, lubrication, tone, and boundaries that helpFascia's surprising role (yes, your bladder “talks” to your neck)Links & resourceshttps://www.tightenyourtinkler.com/ (listener code Michele for $50 off)https://www.instagram.com/tighten.your.tinkler/ Tighten Your Tinkler free quiz https://www.surveymonkey.com/r/tinklerquizIf this helped, share it with a friend, rate the show, and hop on my weekly newsletter for midlife health, fitness, and no-BS motivation._________________________________________1:1 health and nutrition coaching or Faster Way - Reach me anytime at mailto:mfolanfasterway@gmail.com If you're doing “all the right things” and still feel stuck, it may be time to look deeper. I've partnered with EllieMD, a trusted telehealth platform offering modern solutions for women in midlife—including micro-dosed GLP-1 peptide therapy—to support metabolic health and longevity. https://elliemd.com/michelefolan - Create a free account to view all products. ✨ Sign up for my weekly newsletter: https://michelefolanfasterway.myflodesk.com/i6i44jw4fq

As little as 3000 steps per day can slow progression to Alzheimer's Disease; Self-reports of memory impairment soaring among young people; New study vindicates unprocessed red meat—and even often-vilified processed red meat—for cancer and overall health. Prostate artery embolization (PAE) offers new non-invasive option for men's age-related urinary problems; Targeting the mitochondria and the microbiome for Parkinson's Disease; Popular prostate and hair loss prevention drugs linked to depression and suicide—while Cialis for urinary symptoms may stave off cardiovascular disease; Discovery that a safe, cheap medication may increase survival after breast cancer surgery.

Urinary tract infections — or UTIs — aren't the most glamorous topic, but they're incredibly important, and we just don't talk about them enough. If you've ever had one, you'll know how miserable they can be: the burning, the stinging, those endless trips to the loo, the pain, and that bone-crushing fatigue. They can really knock you sideways.For many women, UTIs become more common — and more stubborn — during perimenopause and menopause.In this episode, I'm joined by the brilliant Helen Lake, a specialist urology nurse, to help us understand why UTIs happen, why they mustn't be ignored, and what you can do about them — from medical treatments to nutrition and supplements.Helen explains everything you need to know about identifying, understanding, and managing UTIs — and hopefully banishing them for good. We cover the key symptoms, prevention strategies like staying hydrated and double-voiding, why test results aren't always conclusive, and when antibiotics are needed. We also look at the role of beneficial bacteria, cranberry and D-mannose, vaginal moisturisers, topical oestrogen, and how to advocate for yourself with your GP.If you've found this episode helpful, please share it with a friend who might benefit too. And if you love The Happy Menopause podcast, I'd be so grateful if you could leave a five-star rating and a quick review on Apple Podcasts — or wherever you like to listen.And don't forget to subscribe, so you don't miss out on upcoming episodes. These small steps make a huge difference to the algorithm, and help more women find the show.After all, every woman deserves to have a happy menopause.Check out the full Show Notes for this episode on my website www.well-well-well.co.uk/podcast, where you'll find all the relevant links and references for each guest. Learn how to build your own menopause diet to manage your symptoms with my book The Happy Menopause: Smart Nutrition to Help You Flourish. And if you're tired of feeling tired and grappling with brain fog, check out my new book: The Happy Menopause Guide to Energy; Nutrition to Rejuvenate Your Brain & Body. It's available in all the usual places.

Urinary incontinence and sexual dysfunction are common side effects of prostate cancer treatment, but both are manageable. Dr. Lindsay Hampson explains the types of incontinence—stress, urge, mixed, and overflow—and how identifying the cause guides treatment. Management strategies include pelvic floor physical therapy, medications, and surgical options like slings or artificial urinary sphincters. For sexual dysfunction, approaches range from oral medications and vacuum devices to injections and implants. Dr. Michael Rabow also highlights the side effects of androgen deprivation therapy, including fatigue, depression, hot flashes, and cardiovascular risk. He outlines evidence-based strategies—like exercise, cognitive behavioral therapy, and medications—to help preserve well-being and quality of life during treatment. Series: "Prostate Cancer Patient Conference" [Health and Medicine] [Show ID: 40869]

Urinary incontinence affects millions of women, yet many continue to suffer in silence due to stigma or the misconception that it's just a normal part of aging. Bladder control issues can impact women of all ages, and they are highly treatable, and there are real solutions that can help. On this episode of the Healthier You Podcast, Dr. Ashlee Williams welcomes Dr. Nwamaka Fadahunsi, a board-certified urologist at Kaiser Permanente, to discuss the causes of urinary incontinence and the many tools available to treat it. Dr. Fadahunsi explains the differences between stress and urge incontinence, debunks common myths, and offers practical guidance on what women can do at home. She also outlines the full range of treatment options, including physical therapy, medications, and outpatient procedures, helping women regain control and confidence without relying on pads or assuming surgery is the only answer. Learn more about Nwamaka Fadahunsi, MD
In this very special 100th episode of the Cat Café Podcast, Dr. Susan and Dr. Jolle take a cozy walk down memory lane — catnip lattes in hand — to celebrate a century of cat conversations!

Urinary incontinence is more common than you think. It's rarely talked about. Dr. Nigel Bayer sheds light on this often-ignored issue, offering real solutions to help women restore confidence and improve their quality of life. In this episode, we explore: The root causes of urinary incontinence—and why conventional advice like Kegels or medication often falls short. The Iron Clad Bladder System, an innovative approach using neuroplasticity and nervous system retraining for lasting results. Practical, holistic strategies to improve urinary health naturally without surgery, drugs, or fear of leaks. It's time to take back control. Tune in and discover a new path to freedom! About Dr. BrayerDr. Nigel Brayer, a nationally recognized expert in natural medicine and the creator of the -Iron Clad Bladder System, a groundbreaking, drug-free approach that combines modern neurology and traditional Chinese medicine to heal urinary incontinence. With over 27 years of experience, he has helped countless women overcome this life-altering condition by addressing both the physical symptoms and the deeper neurological and emotional roots of the issue. About TheresaA wife and a mother to two children and grandmother, Theresa Alexander Inman is a Parenting Coach, Board Certified Behavior Analyst, Infant Toddler Development Specialist, Autism Spectrum Disorder Clinical Specialist. Introduced to behavior analysis in 2007 after years in the juvenile justice system.Her goal is to improve the lives of children and families by helping them strategize child develop skills to prevent or reduce the effects of possible delays while having fun! She also served as a panelist on the first annual Autism World Summit.Theresa is also an author, having published “Pathways to Early Communication” in 2022.Connect with Theresa today!• Instagram | Theresa Inman• LinkedIn | Theresa Inman• BabyBoomer.org | Theresa Inman• YouTube | Parenting with Confidence• Tiktok | https://www.tiktok.com/@parentcoachtheresa• Spotify via Anchor.fm | Parenting with Confidence Website: https://www.theresaalexanderinman.com/About Parenting on the SpectrumRaising autistic children comes with unique joys, challenges, and learning moments. Join host Theresa as she explores the diverse experiences of parenting kids on the spectrum. Each episode features expert insights, real-life stories, and practical strategies to help you navigate this journey with understanding, compassion, and strength. Whether you're a parent, caregiver, or ally, this podcast is your go-to resource for fostering connection and celebrating neurodiversity. Please share, comment, rate, and download! Be blissful! Theresa

Send us a textHave you ever wondered why urinary issues seem to affect women differently than men? The answer lies in our unique anatomy and hormonal makeup — factors that make female urinary health both fascinating and complex.Dr. Holly Thacker takes listeners on a comprehensive journey through the most common urologic conditions affecting women during Urology Awareness Month. From the annoying but potentially dangerous urinary tract infections to the embarrassing reality of pelvic organ prolapse that affects up to one in eight women, this episode breaks down what's happening and why."Everyone needs a bladder that works," Dr. Thacker emphasizes as she explores how bladder health connects to overall wellness and quality of life. She tackles taboo topics with medical precision while offering practical advice for prevention and management. You'll learn why maintaining pelvic floor strength matters even if you've never been pregnant, how hormonal changes dramatically affect urologic health, and why sexual function is inextricably linked to bladder health.Subscribe to the Speaking of Women's Health Podcast wherever you listen to podcasts and visit speakingofwomenshealth.com for more resources on taking charge of your health.Support the show

Contributor: Travis Barlock MD Educational Pearls: Meningitis retention syndrome is a relatively novel and rare clinical condition Aseptic meningitis + acute urinary retention One study reports an incidence of about 8% in patients with acute aseptic meningitis Clinical presentation Typical meningeal symptoms including fever, stiff neck, and headache Urinary retention occurs about one week after initial symptoms Potential pathophysiology Immune-mediated dysfunction of the central nervous system Detrusor muscle underactivity from inflammation of the spinal cord Management Supportive care Bladder decompression References Hiraga A, Kuwabara S. Meningitis-retention syndrome: Clinical features, frequency and prognosis. J Neurol Sci. 2018;390:261-264. doi:10.1016/j.jns.2018.05.008 Pellegrino F, Funiciello E, Pruccoli G, et al. Meningitis-retention syndrome: a review and update of an unrecognized clinical condition. Neurol Sci. 2023;44(6):1949-1957. doi:10.1007/s10072-023-06704-0 Summarized & Edited by Jorge Chalit, OMS4 Get your tickets to Tox Talks Event, Sept 11, 2025: https://emergencymedicalminute.org/events-2/ Donate: https://emergencymedicalminute.org/donate/
Real Life Pharmacology - Pharmacology Education for Health Care Professionals
Solifenacin is a bladder antimuscarinic medication most commonly used for overactive bladder (OAB) with symptoms of urinary frequency, urgency, and urge incontinence. Like other agents in its class, understanding the pharmacology can help anticipate potential side effects, drug interactions, and downstream prescribing problems. Mechanism of Action Solifenacin selectively blocks muscarinic M3 receptors in the bladder detrusor muscle. Inhibiting these receptors reduces involuntary bladder contractions, increases bladder capacity, and delays the urge to void. While M3 selectivity may theoretically reduce side effects compared to nonselective antimuscarinics, in clinical practice, many anticholinergic effects still occur. Adverse Effects Because muscarinic receptors are present throughout the body, solifenacin can lead to a range of anticholinergic adverse effects: Dry mouth – among the most common, can be significant enough to cause dental issues with long-term use. Constipation – especially problematic in older adults; severe cases may require hospitalization. Blurred vision – due to impaired accommodation. Cognitive impairment – increased risk in older adults, particularly with cumulative anticholinergic burden. Urinary retention – paradoxical worsening in patients with bladder outlet obstruction. Drug Interactions CYP3A4 inhibitors (e.g., ketoconazole, clarithromycin, ritonavir) can increase solifenacin plasma concentrations, raising the risk of side effects. Other anticholinergics (e.g., diphenhydramine, tricyclic antidepressants, other bladder antimuscarinics) can result in additive toxicity and higher anticholinergic burden. QT-prolonging drugs (e.g., amiodarone, certain fluoroquinolones) may have additive cardiac risk since solifenacin has been associated with QT prolongation in rare cases. Prescribing Cascade Examples Constipation → Laxative initiation – A patient starts solifenacin for OAB and develops severe constipation, leading to chronic use of stimulant laxatives like senna or bisacodyl. Dry mouth → Mouth rinse prescription – Dry mouth is treated with saliva substitutes or prescription rinses, instead of reassessing the anticholinergic therapy. Cognitive decline → Donepezil initiation – In older adults, cognitive impairment may be mistaken for dementia progression, leading to cholinesterase inhibitor prescribing—directly counteracting the anticholinergic effects of solifenacin. Solifenacin can be an effective treatment for OAB, but the risk of adverse effects and prescribing cascades—especially in older adults—cannot be ignored. Healthcare professionals should regularly review the indication, monitor for anticholinergic burden, and look for opportunities to deprescribe when appropriate.
© 2020-2026 Ivy Podcast Discovery LLC
